What medications 💊 are should be avoided 🛑 or used with caution ⚠️ in patients with Myasthenia Gravis? 🤔
See 👀 the thread 🧵below⤵️ that summarizes an amazing grand rounds presentation by @UKPharmRes PGY1 @AliW_PharmD on key 🔑 medication considerations in MG
See 👀 the thread 🧵below⤵️ that summarizes an amazing grand rounds presentation by @UKPharmRes PGY1 @AliW_PharmD on key 🔑 medication considerations in MG

1️⃣Antibiotics to avoid or use w/caution🦠 💊
🛑FQs = FDA BBW for ⤴️ risk of MG crisis ➡️ avoid use if possible
⚠️ Macrolides ⤴️ rate of MG crisis (case reports)
⚠️ AG linked to ⤴️ ICU acquired weakness & exacerbate ‼️ MG crisis
📝Risk⬆️ w/neomycin vs. tobramycin & amikacin
🛑FQs = FDA BBW for ⤴️ risk of MG crisis ➡️ avoid use if possible
⚠️ Macrolides ⤴️ rate of MG crisis (case reports)
⚠️ AG linked to ⤴️ ICU acquired weakness & exacerbate ‼️ MG crisis
📝Risk⬆️ w/neomycin vs. tobramycin & amikacin



Antibiotics considered to be SAFE alternatives to the above include
✅Beta-lactams
✅Tetracyclines
✅Linezolid
✅Bactrim
Ex. In an MG patient who presents 🏥 w/CAP 🫁 ➡️ choose ceftriaxone + doxycycline✅ OVER ceftriaxone + azithromycin🛑
✅Beta-lactams
✅Tetracyclines
✅Linezolid
✅Bactrim
Ex. In an MG patient who presents 🏥 w/CAP 🫁 ➡️ choose ceftriaxone + doxycycline✅ OVER ceftriaxone + azithromycin🛑

2️⃣What about neuromuscular blockers?? 🤔
💉 Succinylcholine requires FUNCTIONAL receptors for activity ▶️ ⬆️⬆️doses in MG
💉 Non-depolarizing agents depend on QUANTITY of receptors ▶️⬇️⬇️doses in MG
⏰ Anticipate PROLONGED DOA for both agents ‼️
💉 Succinylcholine requires FUNCTIONAL receptors for activity ▶️ ⬆️⬆️doses in MG
💉 Non-depolarizing agents depend on QUANTITY of receptors ▶️⬇️⬇️doses in MG
⏰ Anticipate PROLONGED DOA for both agents ‼️

3️⃣Is MAGNESIUM 💉 safe to use in MG? 🤔
⚠️ Mg+2 acts at the NMJ and can ⤴️ muscle weakness & induce 🫁 decompensation in MG
🔑 pearls include transitioning to PO 💊 formulation when appropriate & consider a LOWER Mg level threshold for replacement ❗️
⚠️ Mg+2 acts at the NMJ and can ⤴️ muscle weakness & induce 🫁 decompensation in MG
🔑 pearls include transitioning to PO 💊 formulation when appropriate & consider a LOWER Mg level threshold for replacement ❗️

4️⃣Final class of agents included beta blockers 💊 🫀
⛔️ BB have been dose-dependent ⬇️ in NM transmission in 🐀 models
However this is MORE likely to occur with lipophilic agents such as propranolol vs. metoprolol/atenolol
✅Monitor for muscle weakness
⛔️ BB have been dose-dependent ⬇️ in NM transmission in 🐀 models
However this is MORE likely to occur with lipophilic agents such as propranolol vs. metoprolol/atenolol
✅Monitor for muscle weakness

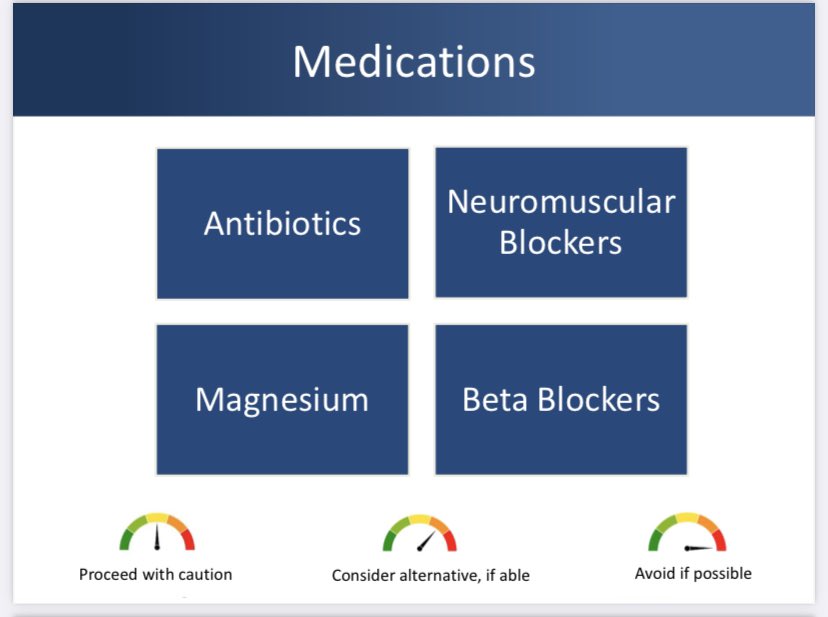
⭐️ Summary slide on medication classes considered to avoid 🛑 use with caution (orange)⚠️ or considered to be OK as long as monitored (yellow) in MG.
Pharmacists 👩🏻⚕️ are 🔑 to mitigate risk of exacerbating neuromuscular toxicity in patients with MG! #TwitteRx #PharmICU
Pharmacists 👩🏻⚕️ are 🔑 to mitigate risk of exacerbating neuromuscular toxicity in patients with MG! #TwitteRx #PharmICU


• • •
Missing some Tweet in this thread? You can try to
force a refresh