A #tweetorial #medtweetorial
@MedTweetorials
1/
3 AM: Pager Pager Pager
Me [very groggily]: Hey, what’s up?
Awesome overnight APP: Sorry to wake you! But, Mrs. Very-Small-Stroke-NIHSS-2-Had-Been-Clinically-Stable-All-Day just PEA arrested.
Me [not so groggily]:
@MedTweetorials
1/
3 AM: Pager Pager Pager
Me [very groggily]: Hey, what’s up?
Awesome overnight APP: Sorry to wake you! But, Mrs. Very-Small-Stroke-NIHSS-2-Had-Been-Clinically-Stable-All-Day just PEA arrested.
Me [not so groggily]:
2/
Awesome APP: We successfully got ROSC (bc team
@emoryneurocrit
= Flexed bicepsStar-struck) and have him stabilized. Going to scan now!
So, #neurotwitter, where’s the lesion?
Awesome APP: We successfully got ROSC (bc team
@emoryneurocrit
= Flexed bicepsStar-struck) and have him stabilized. Going to scan now!
So, #neurotwitter, where’s the lesion?
3/
Trick question.
All of these areas through neurologic pathology – stroke/seizure/bleed - could all have caused a sudden death (or at the very least sudden LOC).
Trick question.
All of these areas through neurologic pathology – stroke/seizure/bleed - could all have caused a sudden death (or at the very least sudden LOC).
4/
For example, seizures originating from the left insula can result in prolonged QT and Upwards arrow risk of ventricular arrhythmias
Epileptic events from the right insula can result in shortening of the QT interval & Upwards arrow the risk of vagally mediated syncope.
For example, seizures originating from the left insula can result in prolonged QT and Upwards arrow risk of ventricular arrhythmias
Epileptic events from the right insula can result in shortening of the QT interval & Upwards arrow the risk of vagally mediated syncope.
5/
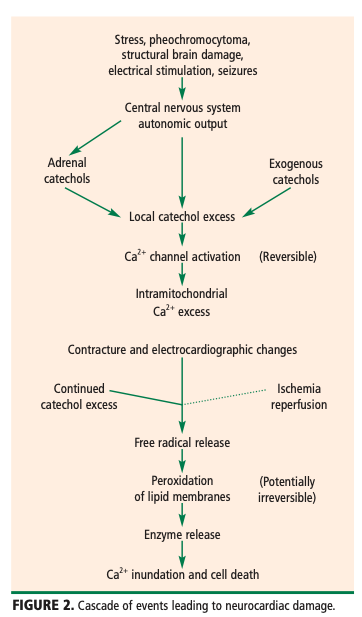
Perhaps there is nothing in med more fascinating than the brain-cardiac connection mediated by the autonomic nervous system beautifully elucidated by
@BWHNeurology
neurologist extraordinaire Marty Samuels in his paper “The Voodoo Death Revisited”
Perhaps there is nothing in med more fascinating than the brain-cardiac connection mediated by the autonomic nervous system beautifully elucidated by
@BWHNeurology
neurologist extraordinaire Marty Samuels in his paper “The Voodoo Death Revisited”
6/
Thanks @AaronLBerkowitz for sharing the PDF w/ me!
This is the paper, but the DOI won't link Disappointed but relieved faceif anyone else has a working link, pls share in comments!
'Voodoo' death revisited: the modern lessons of neurocardiology
pubmed.ncbi.nlm.nih.gov
Thanks @AaronLBerkowitz for sharing the PDF w/ me!
This is the paper, but the DOI won't link Disappointed but relieved faceif anyone else has a working link, pls share in comments!
'Voodoo' death revisited: the modern lessons of neurocardiology
pubmed.ncbi.nlm.nih.gov
7/
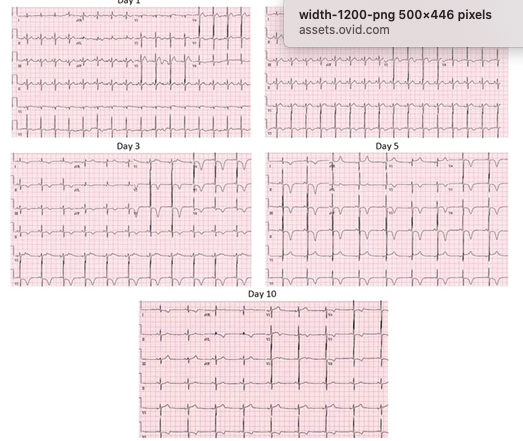
We see many of these catecholamine-driven changes in SAH pts: QT prolongation (common!), cerebral “T waves,” ventricular arrythmias, Takotsubo-cardiomyopathy 💔.
Just another plug for a career in #neurocriticalcare
Cerebral T Waves from RMCA stroke tinyurl.com/fcttjfw8
We see many of these catecholamine-driven changes in SAH pts: QT prolongation (common!), cerebral “T waves,” ventricular arrythmias, Takotsubo-cardiomyopathy 💔.
Just another plug for a career in #neurocriticalcare
Cerebral T Waves from RMCA stroke tinyurl.com/fcttjfw8
8/
But in this case, the acute arrest was the result of something else.
Our pt presented after several hours of acute hoarseness, dysphagia, and “feeling off balanced” (lateropulsion).
Neuro exam= miosis of the L pupil & slight ptosis+L ataxia.
CTA= occluded V4 on the L.
But in this case, the acute arrest was the result of something else.
Our pt presented after several hours of acute hoarseness, dysphagia, and “feeling off balanced” (lateropulsion).
Neuro exam= miosis of the L pupil & slight ptosis+L ataxia.
CTA= occluded V4 on the L.
9/
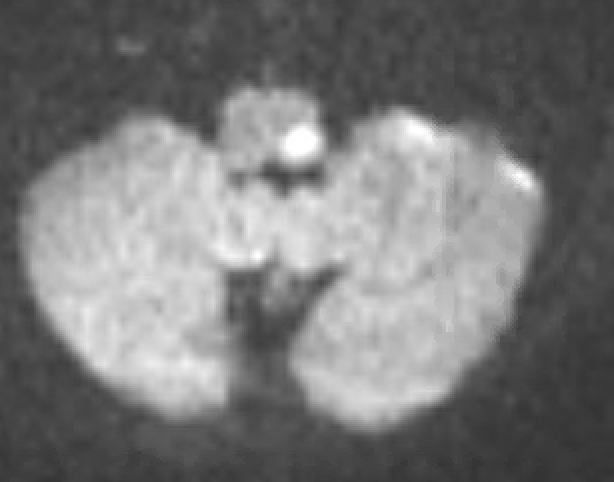
Thought Wallenberg? Correct!
MRI revealed a sizable lateral medullary infarct and her syndrome is a partial Wallenberg syndrome.
Image
Thought Wallenberg? Correct!
MRI revealed a sizable lateral medullary infarct and her syndrome is a partial Wallenberg syndrome.
Image
10/
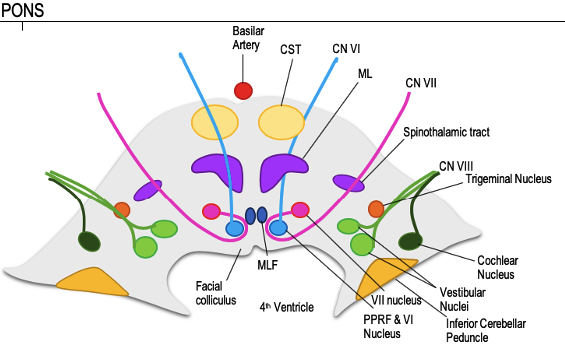
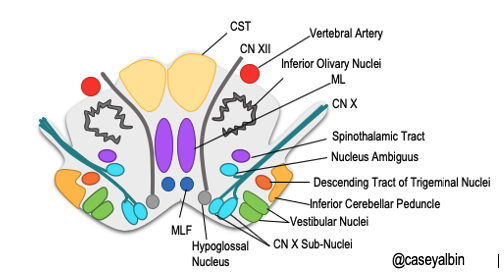
As you’ll remember from the brainstem segments in the #AcuteNeurologySurvivalGuide, there are a lot of important brainstem nuclei in the medulla, but what’s not included here are the neurons that generate breathing.
Diagram of #medulla oriented to the MRI/CT image:
As you’ll remember from the brainstem segments in the #AcuteNeurologySurvivalGuide, there are a lot of important brainstem nuclei in the medulla, but what’s not included here are the neurons that generate breathing.
Diagram of #medulla oriented to the MRI/CT image:
11/
So, neurologically-speaking, how do we breathe?
The mechanisms underlying this vital function are partially understood. Much of what we know originated by sectioning brainstems of cats (sry it’s true).
@SamBSnider
I remember your awesome noon conference about this!
So, neurologically-speaking, how do we breathe?
The mechanisms underlying this vital function are partially understood. Much of what we know originated by sectioning brainstems of cats (sry it’s true).
@SamBSnider
I remember your awesome noon conference about this!
12/
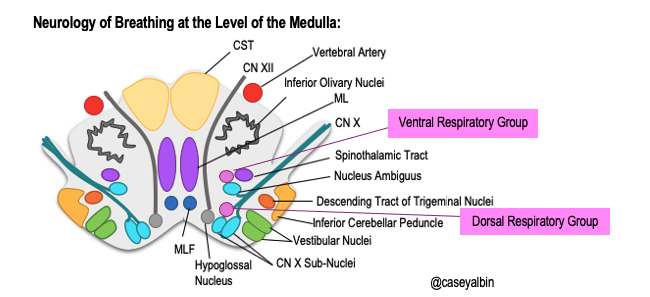
Each half of the brainstem is capable of producing an independent respiratory rhythm, and groups of nuclei in the pons and medulla bilaterally are part of the complex process that governs the oscillation between inspiration and expiration
Each half of the brainstem is capable of producing an independent respiratory rhythm, and groups of nuclei in the pons and medulla bilaterally are part of the complex process that governs the oscillation between inspiration and expiration
13/
These nuclei are:
1⃣ Ventral respiratory group (VRG) including pre-Botzinger complex (near nuc. Ambiguus up to the level of the facial nucleus rostrally)
2⃣ Dorsal medullary RG (DRG) – near nuc. Tractus Solidarius
3⃣ Clusters of cells in the dorsolateral pons (PRG)
These nuclei are:
1⃣ Ventral respiratory group (VRG) including pre-Botzinger complex (near nuc. Ambiguus up to the level of the facial nucleus rostrally)
2⃣ Dorsal medullary RG (DRG) – near nuc. Tractus Solidarius
3⃣ Clusters of cells in the dorsolateral pons (PRG)
14/
When these areas are impaired, hypoventilation may occur when the pt is awake, but much more commonly apnea and hypoventilation occur in sleep.
This is known as Central Hypoventilation Syndrome (CHS) or... Ondine's Curse....
When these areas are impaired, hypoventilation may occur when the pt is awake, but much more commonly apnea and hypoventilation occur in sleep.
This is known as Central Hypoventilation Syndrome (CHS) or... Ondine's Curse....
15/
The name Ondine’s curse references the German myth of a sea nymphFairy(Ondine) who condemns her adulterous lover to loss of all movements that do not require conscious will.
The name Ondine’s curse references the German myth of a sea nymphFairy(Ondine) who condemns her adulterous lover to loss of all movements that do not require conscious will.
16/
Stroke is the most common cause of *acquired* CHS, and usually results from an occlusion in the distal vert (L > R although this is debated). PICA occlusions also described. tinyurl.com/wjs35c69 & tinyurl.com/tcz5ajch.
Non-vascular mech such as poliomyelitis= rare
Stroke is the most common cause of *acquired* CHS, and usually results from an occlusion in the distal vert (L > R although this is debated). PICA occlusions also described. tinyurl.com/wjs35c69 & tinyurl.com/tcz5ajch.
Non-vascular mech such as poliomyelitis= rare
17/
This awesome paper used lesion network-symptom-mapping of 16 patients with CHS and 32 controls with Lateral Medullary Infarcts to show a significant association of the ventro-lateral region of the rostral medulla.
Network Localization of CHS in LMS tinyurl.com/twjv7n38
This awesome paper used lesion network-symptom-mapping of 16 patients with CHS and 32 controls with Lateral Medullary Infarcts to show a significant association of the ventro-lateral region of the rostral medulla.
Network Localization of CHS in LMS tinyurl.com/twjv7n38

18/
How do I know that that’s what happened hereThinking face ?
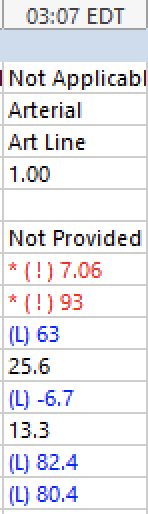
Well ECHO was remarkable only for LVH, tele with no evidence of arrhythmia/ischemia, and her ABG taken a several minutes after being started intubated and ventilated demonstrated this:
pH 7.06 and PaCO2 of 93!
How do I know that that’s what happened hereThinking face ?
Well ECHO was remarkable only for LVH, tele with no evidence of arrhythmia/ischemia, and her ABG taken a several minutes after being started intubated and ventilated demonstrated this:
pH 7.06 and PaCO2 of 93!
19/
Fortunately, after several days of mechanical ventilation she was able to tolerate PSV without apneic spells and was extubated to BIPAP and then transitioned to only nocturnal BIPAP.
Fortunately, after several days of mechanical ventilation she was able to tolerate PSV without apneic spells and was extubated to BIPAP and then transitioned to only nocturnal BIPAP.
20/
Treatment of her acute vertebral occlusion was managed with DAPT.
(Hi, this week’s @JAMAneurology visual abstract, I Eyes you).
No further ischemia was detected, but unfortunately she suffered a GI bleed.
DAPT vs ASA in Patients With Stroke or TIA
tinyurl.com/3ajz9s62
Treatment of her acute vertebral occlusion was managed with DAPT.
(Hi, this week’s @JAMAneurology visual abstract, I Eyes you).
No further ischemia was detected, but unfortunately she suffered a GI bleed.
DAPT vs ASA in Patients With Stroke or TIA
tinyurl.com/3ajz9s62
21/
So, the take-aways here?
⭐️Lateral medullary strokes may result in Central Hypoventilation Syndrome & resultant circulatory collapse!
⭐️Neurology of Breathing: Ventral respiratory group (VRG) including pre-Botzinger complex, Dorsal RG (DRG), and pontine RR (PRG)
⭐️Ondine...
So, the take-aways here?
⭐️Lateral medullary strokes may result in Central Hypoventilation Syndrome & resultant circulatory collapse!
⭐️Neurology of Breathing: Ventral respiratory group (VRG) including pre-Botzinger complex, Dorsal RG (DRG), and pontine RR (PRG)
⭐️Ondine...
22/ Love your thoughts/experience! @Capt_Ammonia @AaronLBerkowitz @namorrismd @nsanar @pouyeah @feras_akbik @rwregen @aszelikovich @wesleytkerr @vascularnotes @CPSolvers @sauravmed @guroledip @AlexReynoldsMD @WNGtweets @NMatch2022 @SitaraKoneru @JackieKraft4 @justine_ker @dbfisch
@EricLawson90 @Nirav_r_bhatt @EmoryNeurology @EmoryNeurohosp1 @RebeccaFasanoMD @Tracey1milligan @SubinMatthews
FYI in the first version of this posted, Twitter only displayed 1/-9/, so when I frantically copy/re-entered it, some of the emojis were copied as their description....Which is actually quite comical. Know there were some 💪🏻🤩, (not ‘flexed bicep superstar eyes’) 😂😂
• • •
Missing some Tweet in this thread? You can try to
force a refresh