THREAD on latest Covid situation in the UK:
TLDR things are looking pretty good right now. Caveat is variants (which is a whole other thread). 1/16
TLDR things are looking pretty good right now. Caveat is variants (which is a whole other thread). 1/16
Overall UK cases are hoevering at just over 2K a day and back to levels back at the end of last summer. We can see drop over Easter hols (partly due to less testing) - but clear that opening outdoor spaces & shops has not caused an uptick (good!!). 2/16 

Looking at types of tests done, clear upticks in twice weekly rapid LFDs when schools are open.
The drop off in LFDs over last few weeks also obv. School kids doing them less? other people? no idea. But clearly govt aim for loads of people to do them not happening. 3/16
The drop off in LFDs over last few weeks also obv. School kids doing them less? other people? no idea. But clearly govt aim for loads of people to do them not happening. 3/16

Worryingly, the proportion of positive cases that are rapid tests *unconfirmed* by PCR tests has gone up (70% of LFD +ves!) - even though confirmatory PCR is available. Why? Who? Means it's hard to know how to interpret case numbers. 4/16

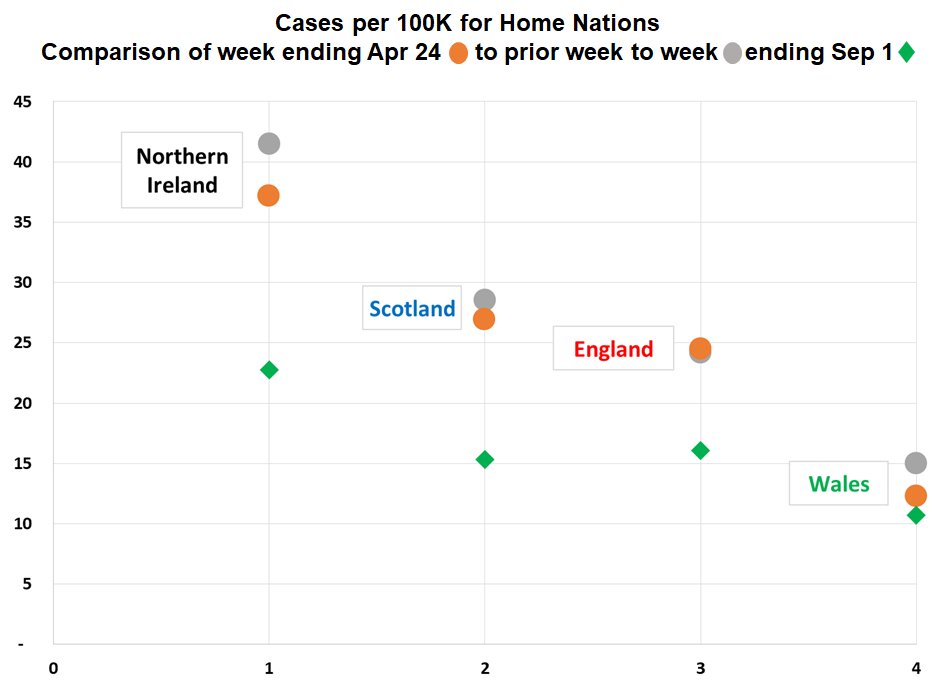
Still, looking at positivity rates for each nation (PCR tests only), clear that positivity is reducing and back at levels last seen summer 2020. ONS infection survey has same picture.
This is a good thing. 5/16
This is a good thing. 5/16

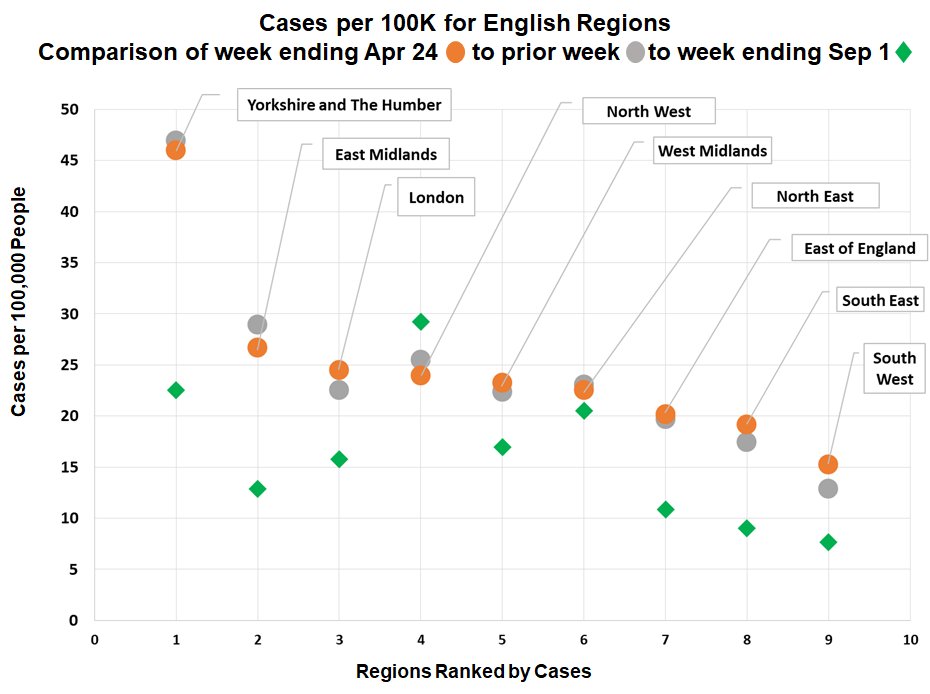
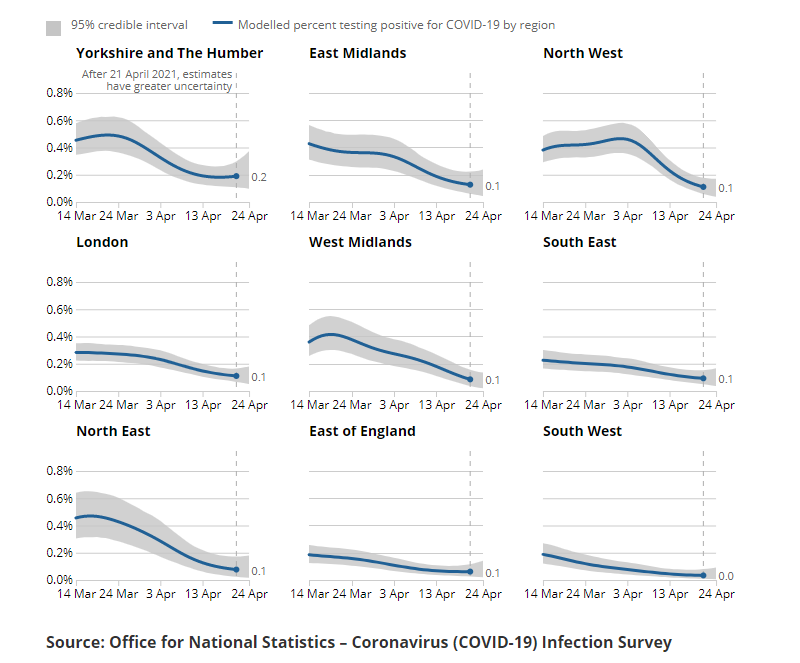
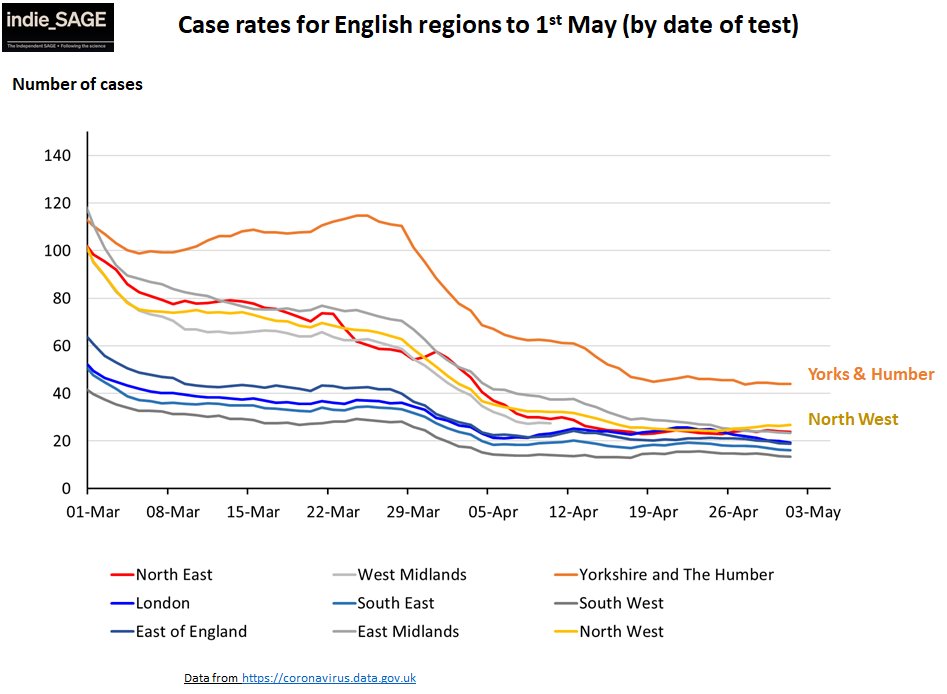
Regionally in England, Yorks & Humber still has highest rates (ONS agrees). Slight increase in NW. Everywhere else flat or declining. ONS says similar but says London, Yorks, East of England might not be declining. 6/16
Hospitalisations and deaths are both back at levels last seen in the summer. This is a combination of low case rates after months of lockdown *and* highly effective vaccines in over 90% of our most vulnerable people. Excellent. 7/16


We're steady at around 3m jabs a week for vax and still mainly on second doses. Expect this to continue for a few more weeks but we are on track to offer 1st jab to all adults by end July and 2 jabs to all by end Sept. 8/16

Currently we're doing first jabs in the 40s - 75% of 45-49 yr olds already have one. For second jabs we're on the 65-74 yr olds and hopefully finding the last few % of older groups. All good. 9/16

That said, ONS released a comprehensive breakdown by different demographics. Similar to what we've seen from before, lower take up in black & minority ethnic populations, more deprived communities. There seem to be some language barriers too. 10/16



Let's have a closer look at schools... From public health england data, although 10-19 year olds have highest case rates, we have not (yet?) seen the increase in cases we saw in March.
ONS says cases in school age kids falling. 11/16
ONS says cases in school age kids falling. 11/16


PHE also show a small increase in school outbreaks but levels much lower than in March and massively lower than last winter.
This is all good and shows that low levels of Covid in communities + mitigations such as masks can and do make schools safer. 12/16
This is all good and shows that low levels of Covid in communities + mitigations such as masks can and do make schools safer. 12/16

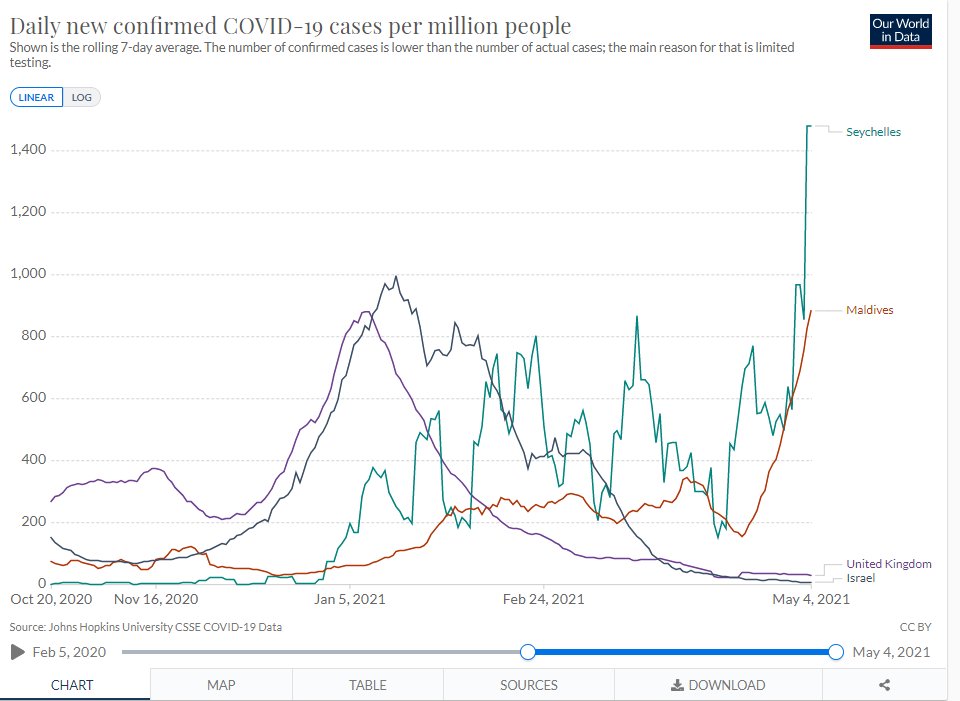
Finally the international picture... Cases globally remain very high. The last week saw the most cases ever recorded. 13/16

Although US is doing ok (although they still have rates 2x ours), Europe is high (even if coming down) & S. America & Asia (driven by India & neighbours) are experiencing terrible Covid surges.
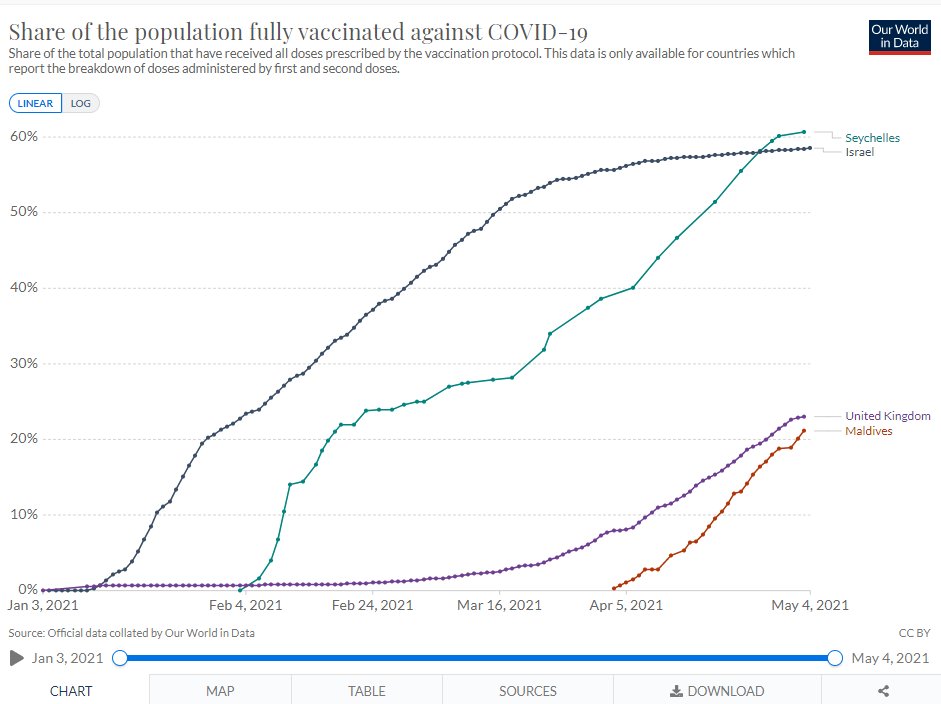
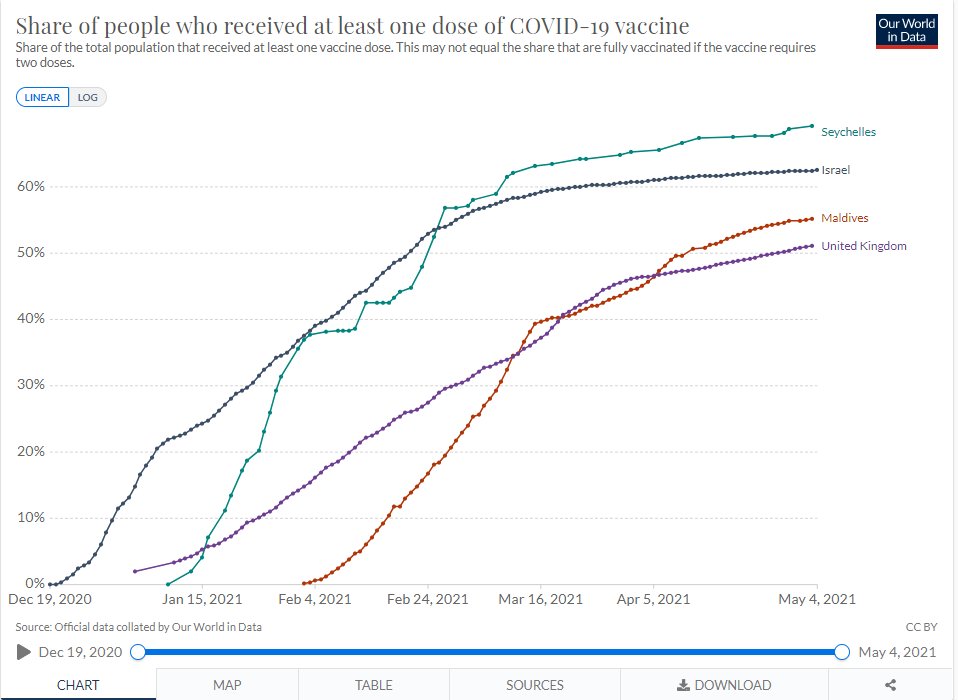
They also have much lower vax rates. Helping vaccinate the globe is crucial! 14/16
They also have much lower vax rates. Helping vaccinate the globe is crucial! 14/16

(NB I've not put on same plot cos denominators not really comparable - Asia looks v low cos such a large pop inc China which is basically zero Covid, S America also has very large and very geographically spread pop). Both also have worse testing. 15/16
Anyway, to sum up everything going in right direction.
I wish I knew who was doing LFDs and why (eg are symptomatic using them instead of PCR cos quicker?)
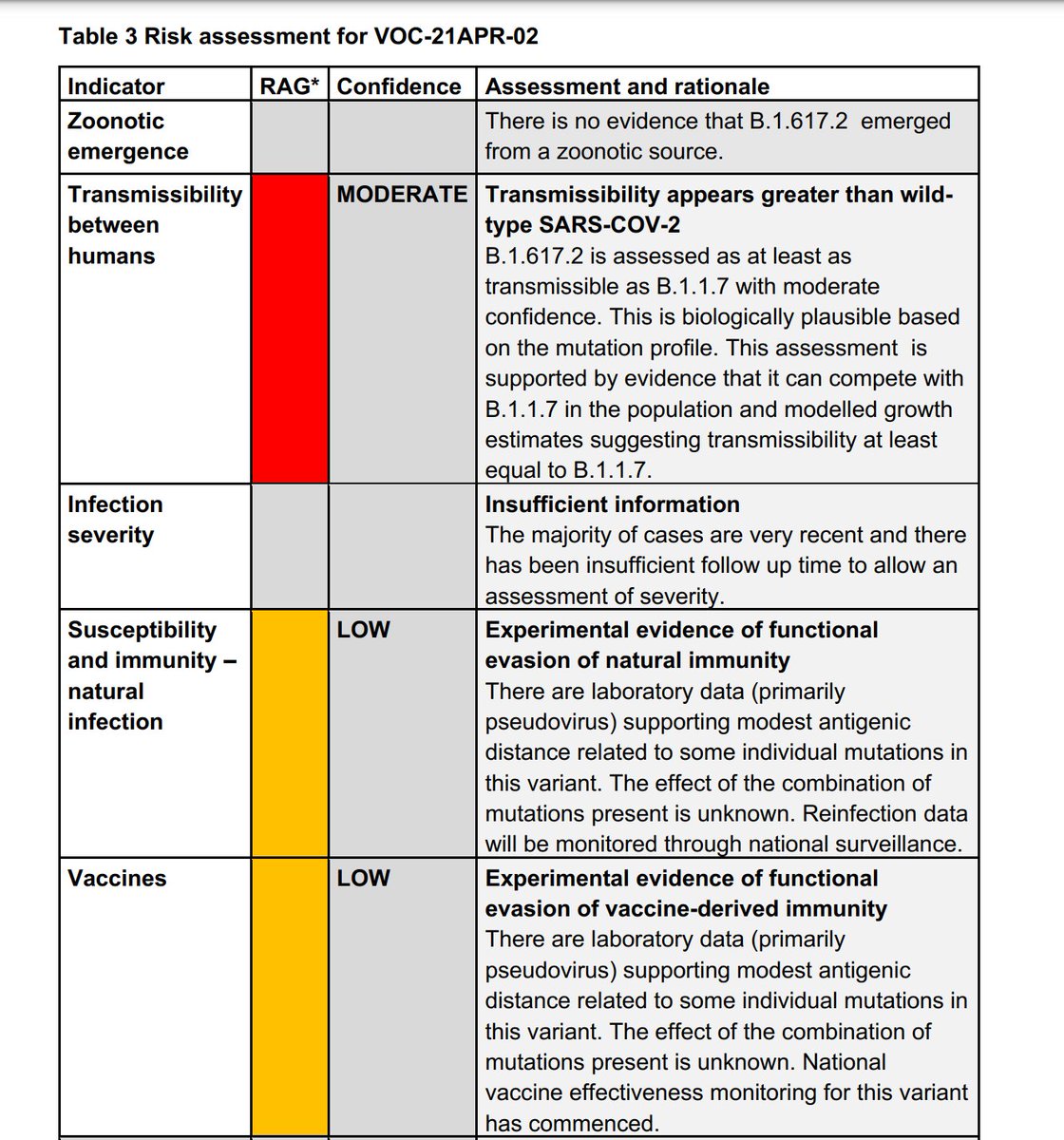
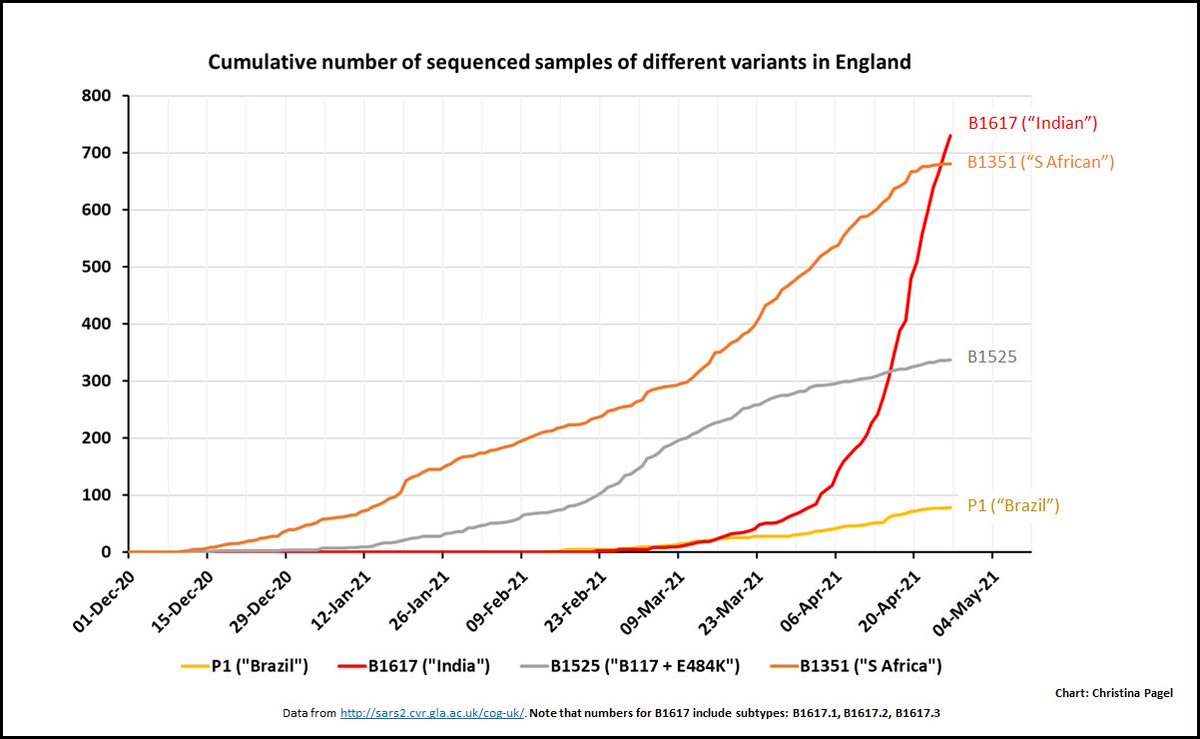
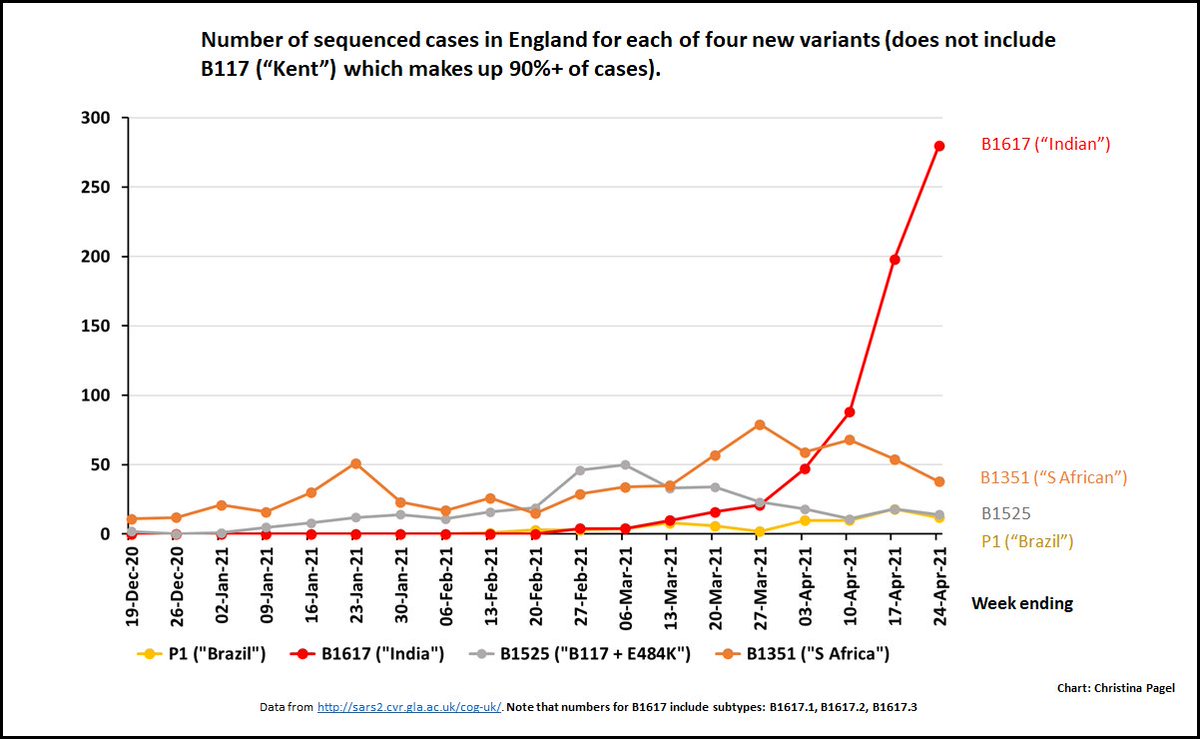
The fly in the ointment is variants - but that's the next thread...
Thx as ever to Bob Hawkins for his help. 16/16
I wish I knew who was doing LFDs and why (eg are symptomatic using them instead of PCR cos quicker?)
The fly in the ointment is variants - but that's the next thread...
Thx as ever to Bob Hawkins for his help. 16/16
• • •
Missing some Tweet in this thread? You can try to
force a refresh