THREAD on new Variant of Concern (VOC), B.1.617.2:
PHE released its report on B.1.617.2. It has loads of info - some quite disturbing.
I'll try to go through the key bits in this thread.
Full doc is here: assets.publishing.service.gov.uk/government/upl…
all graphs use their data. 17 tweets.
PHE released its report on B.1.617.2. It has loads of info - some quite disturbing.
I'll try to go through the key bits in this thread.
Full doc is here: assets.publishing.service.gov.uk/government/upl…
all graphs use their data. 17 tweets.
It's become a VOC because it's been spreading so fast - and in the community.
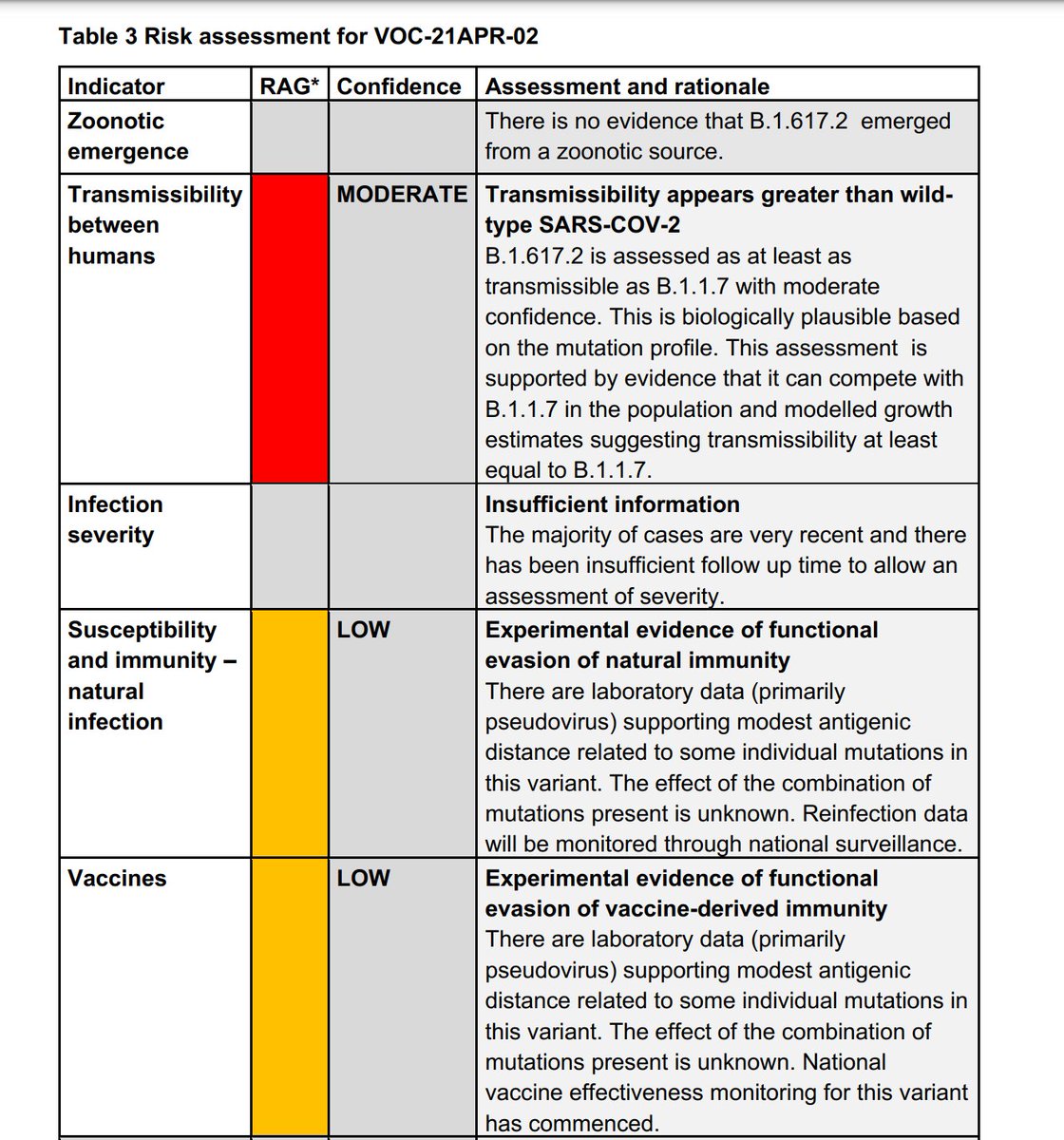
PHE are pretty sure (MODERATE) it's *at least* as transmissible as our dominant "Kent" variant (B117) (RED rating). They are worried (AMBER) it might have some immune escape but don't know yet (LOW)
PHE are pretty sure (MODERATE) it's *at least* as transmissible as our dominant "Kent" variant (B117) (RED rating). They are worried (AMBER) it might have some immune escape but don't know yet (LOW)
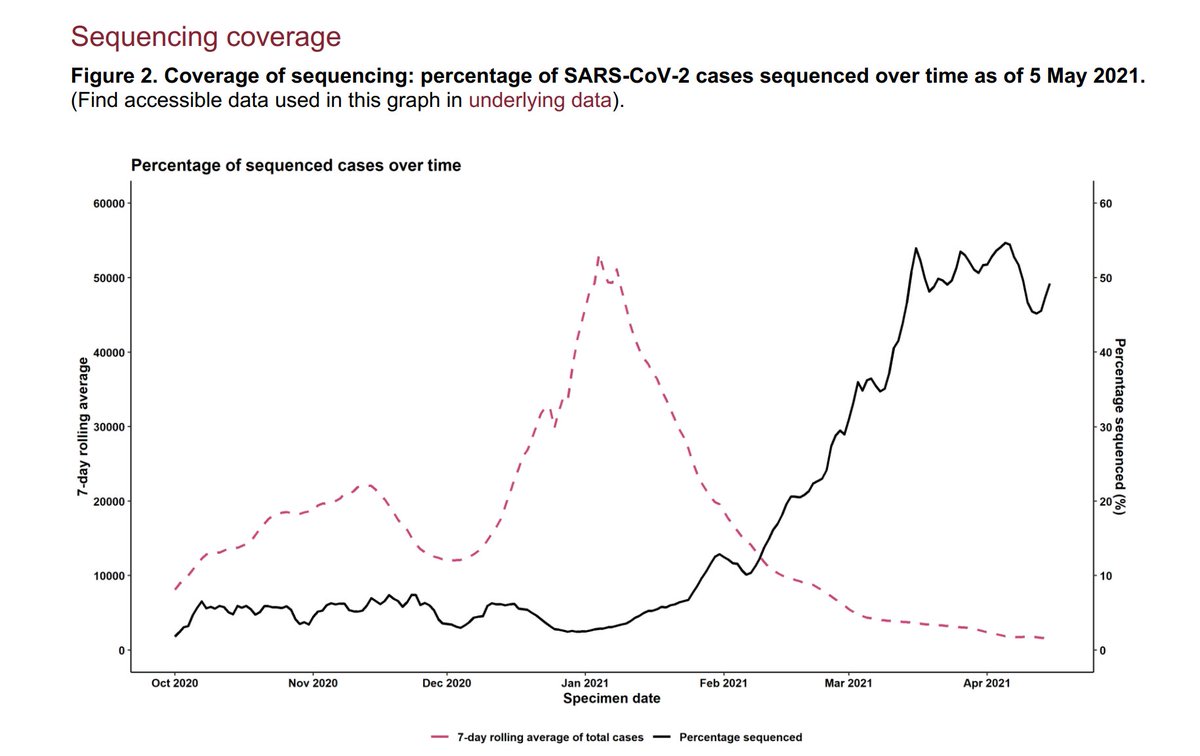
First, note that as overall cases have come down, we're sequencing *more* community cases - since early March about 50% of all postive PCR cases. This means estimates of spread are pretty good. And less bias from traveller data (all traveller +ves sequenced).
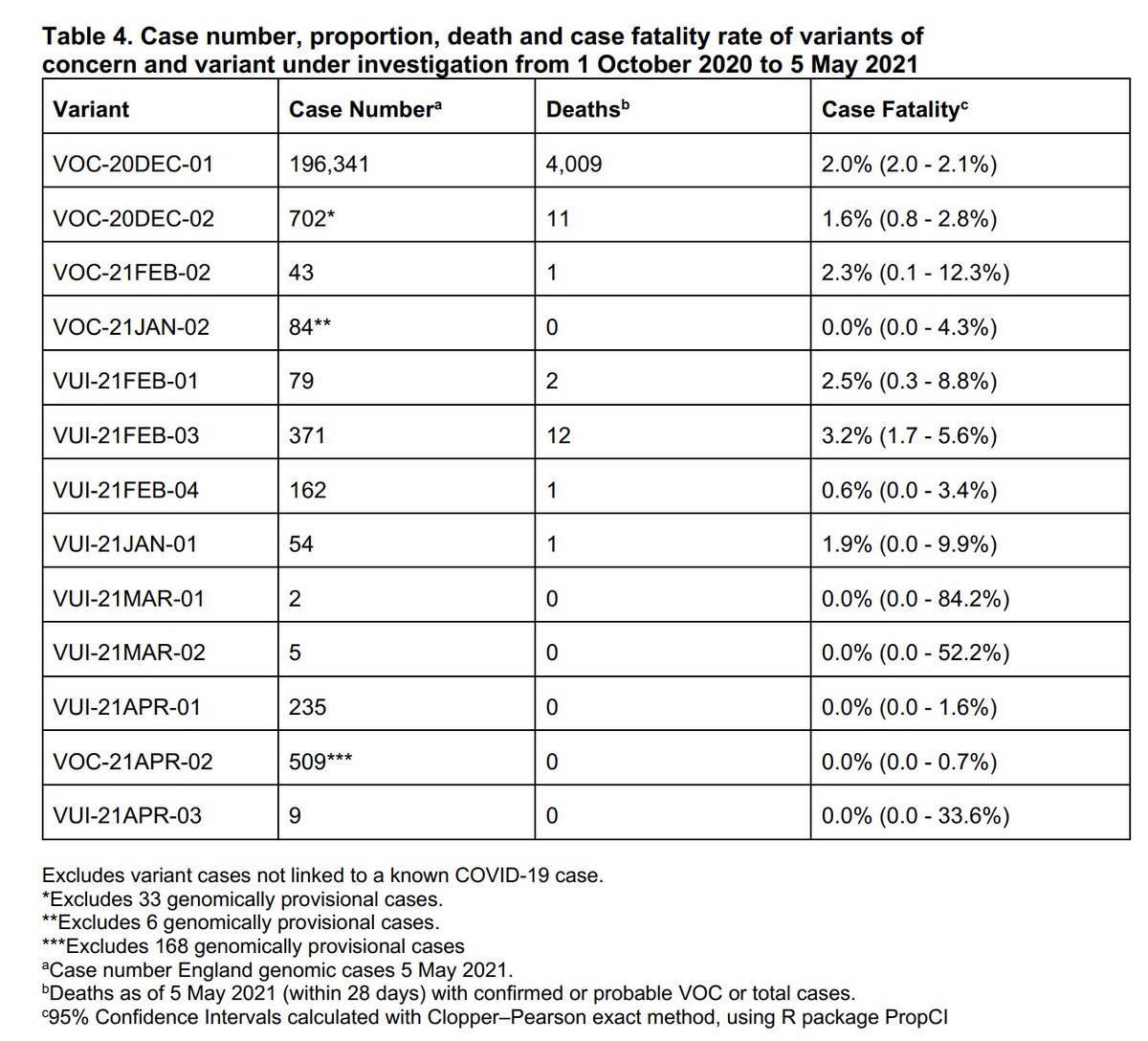
As of 5 May, there have been 509 *confirmed* B.1.617.2 cases in England plus another *168* provisional cases. Together that makes it more numerous than any other variant except dominant Kent.
And all in 4 weeks.
It's too new to say anything about its severity.
And all in 4 weeks.
It's too new to say anything about its severity.
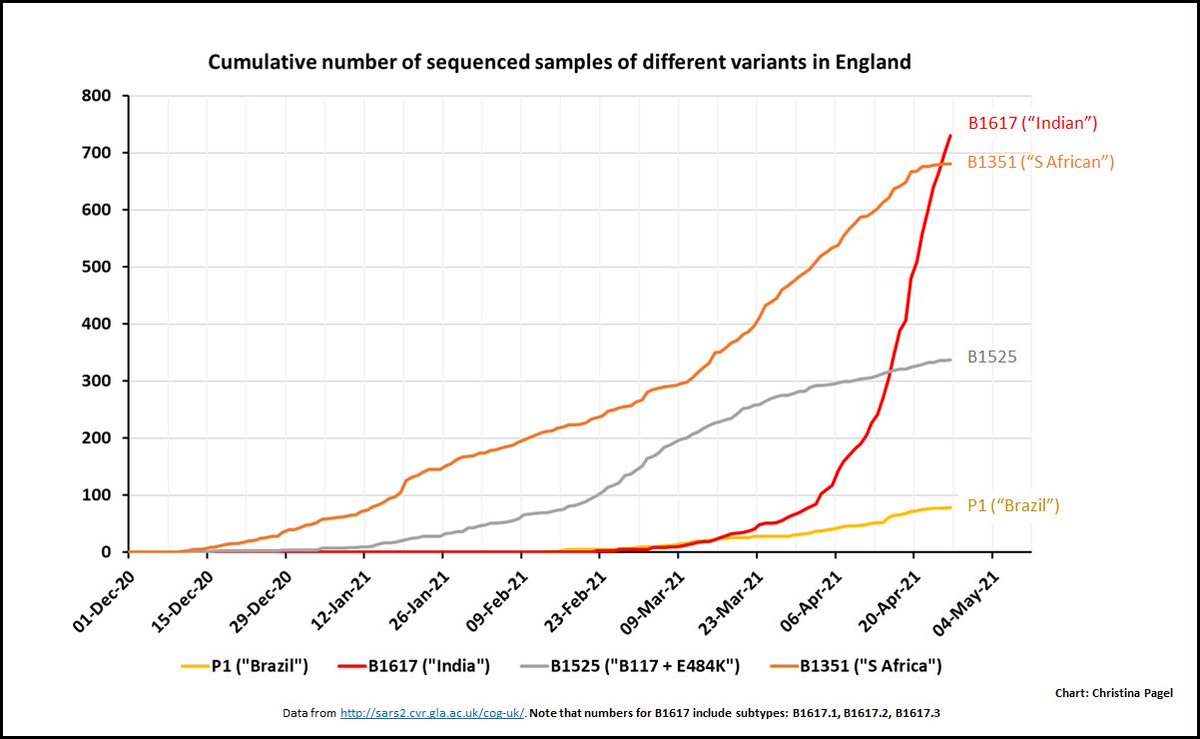
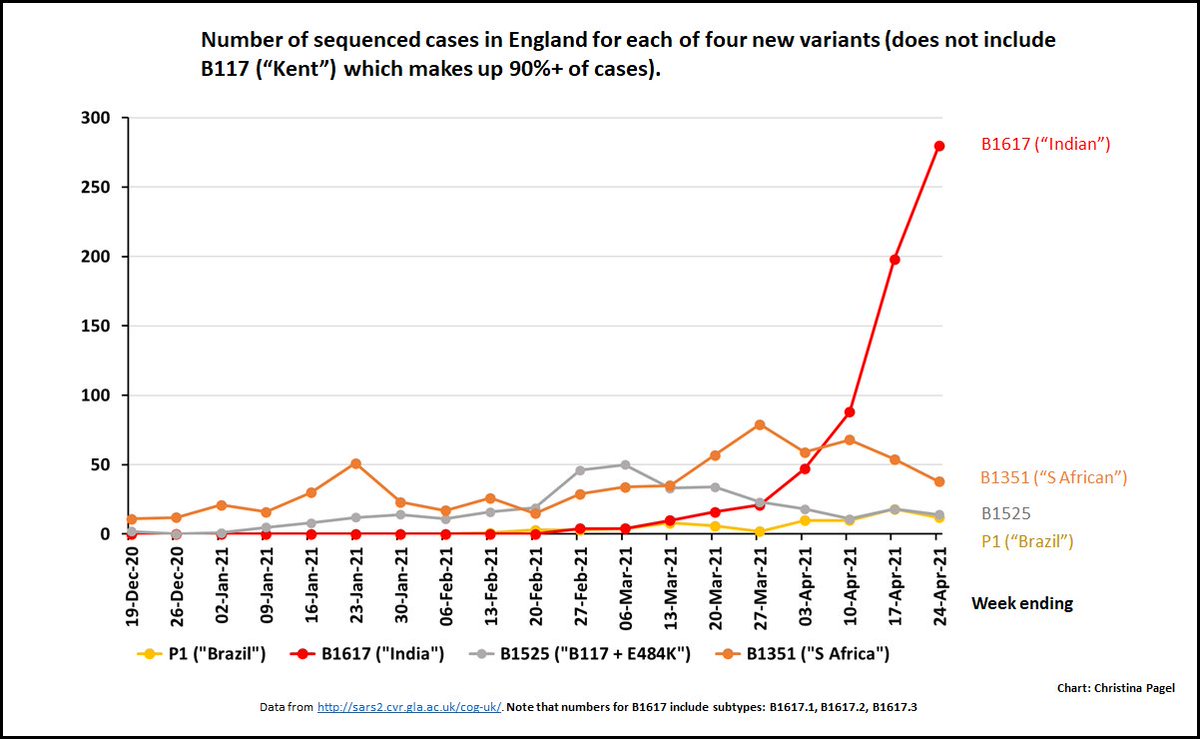
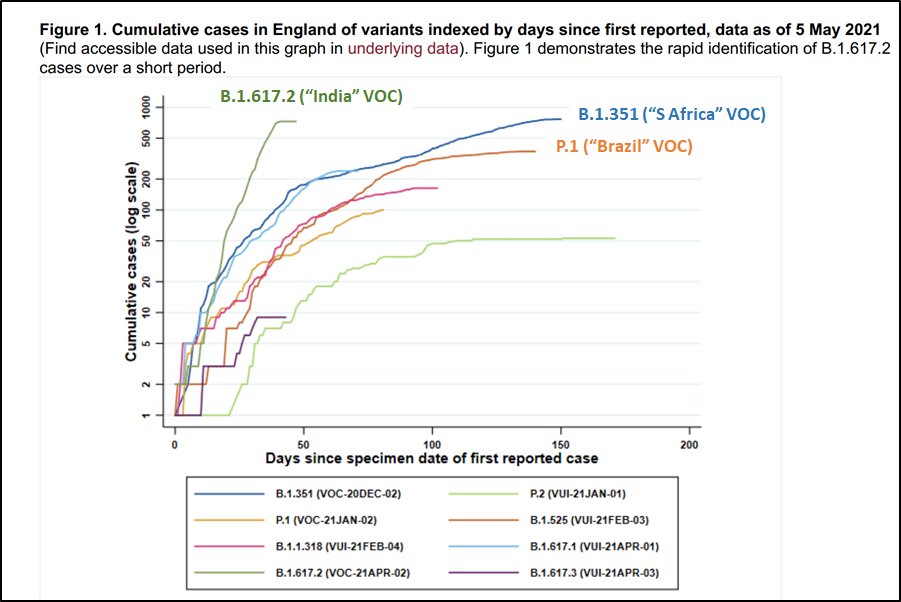
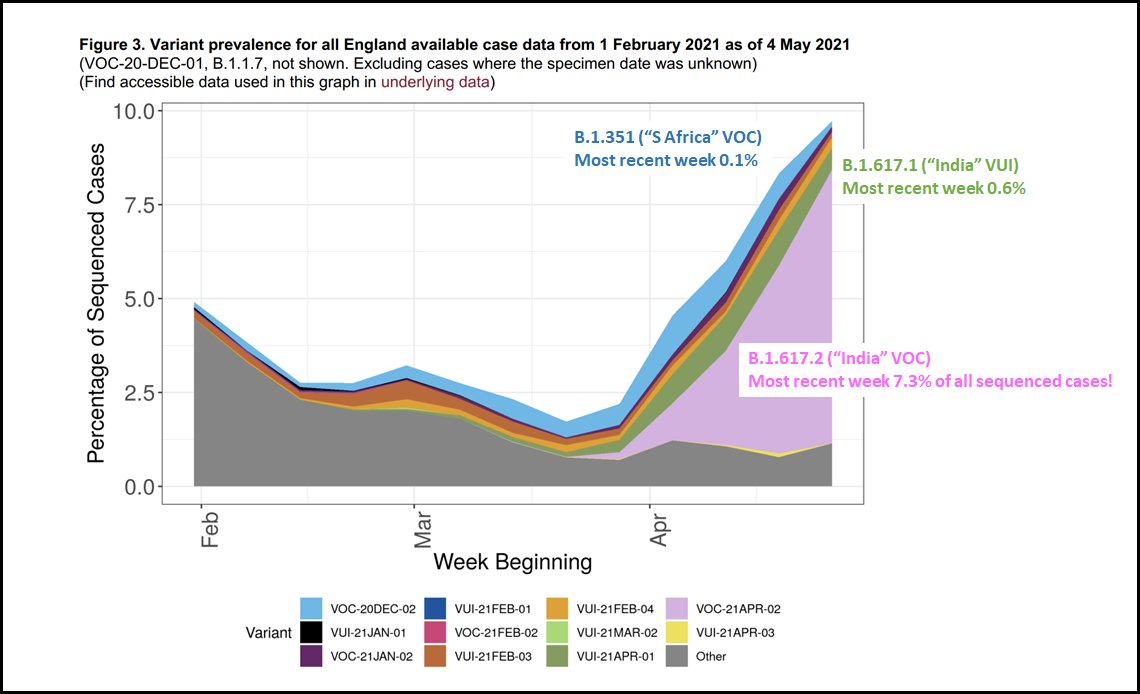
This chart shows how quickly cases of each of the variants have increased from time of first detection in England. The rapidness of B.1.617.2 is evident.
The pale blue line tracking the S Africa rise is B.1.617.1, its slower sibling...
The pale blue line tracking the S Africa rise is B.1.617.1, its slower sibling...
In terms of proportion of all sequenced cases, in the most recent week B.1.617.2 was a whopping 7.3% of all sequenced cases - far outstripping all the other variants. B117 ("Kent") (not shown) is still dominant but losing ground to B.1.617.2.
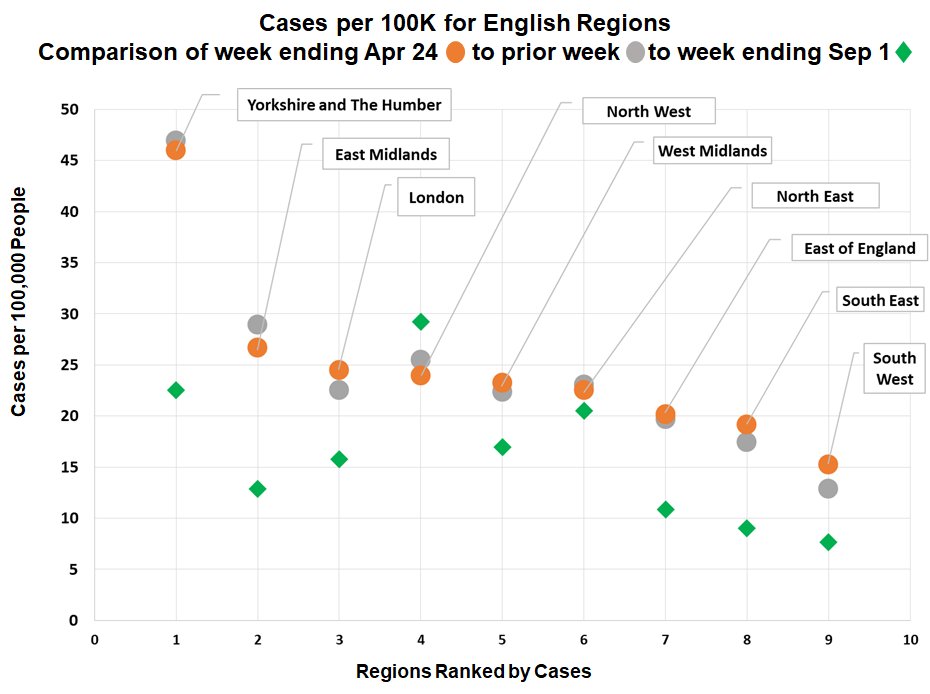
PHE then look for regional variation. B.1.617.2 is not widespread in many regions. I show the highest regions here.
PHE note that SW is high but from v low cases & mostly travellers so I've not shown it
Note most recent weeks have far less data (lag in sequencing). STILL....
PHE note that SW is high but from v low cases & mostly travellers so I've not shown it
Note most recent weeks have far less data (lag in sequencing). STILL....
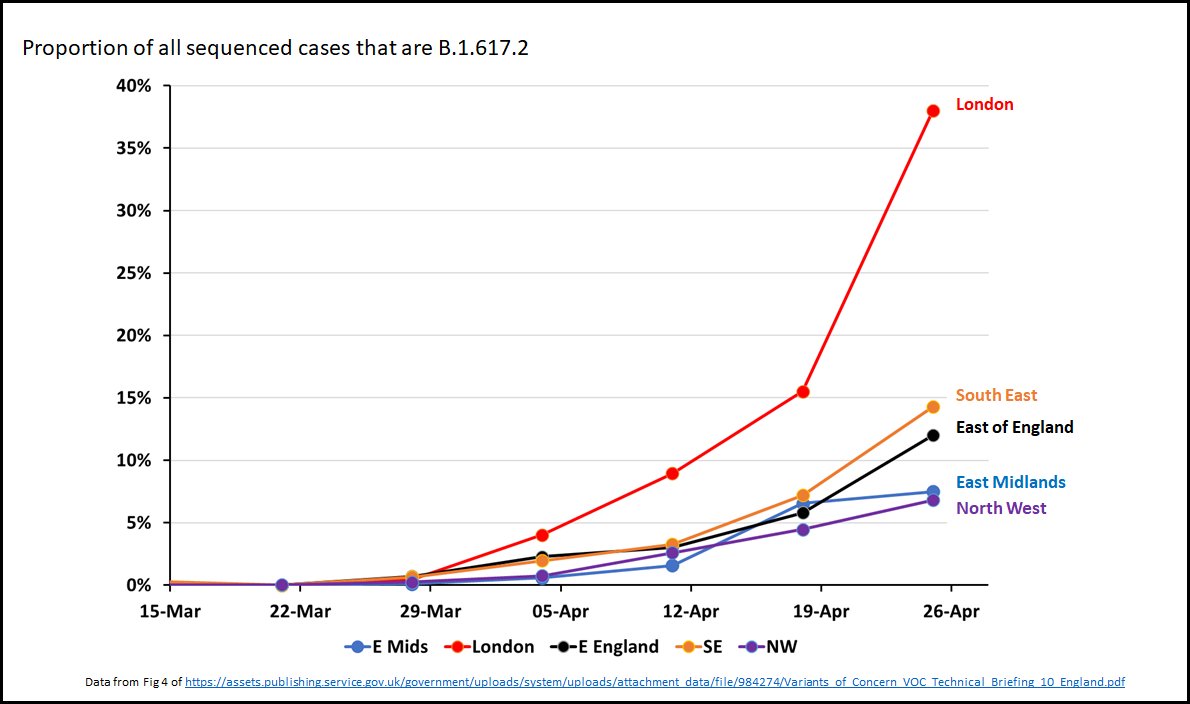
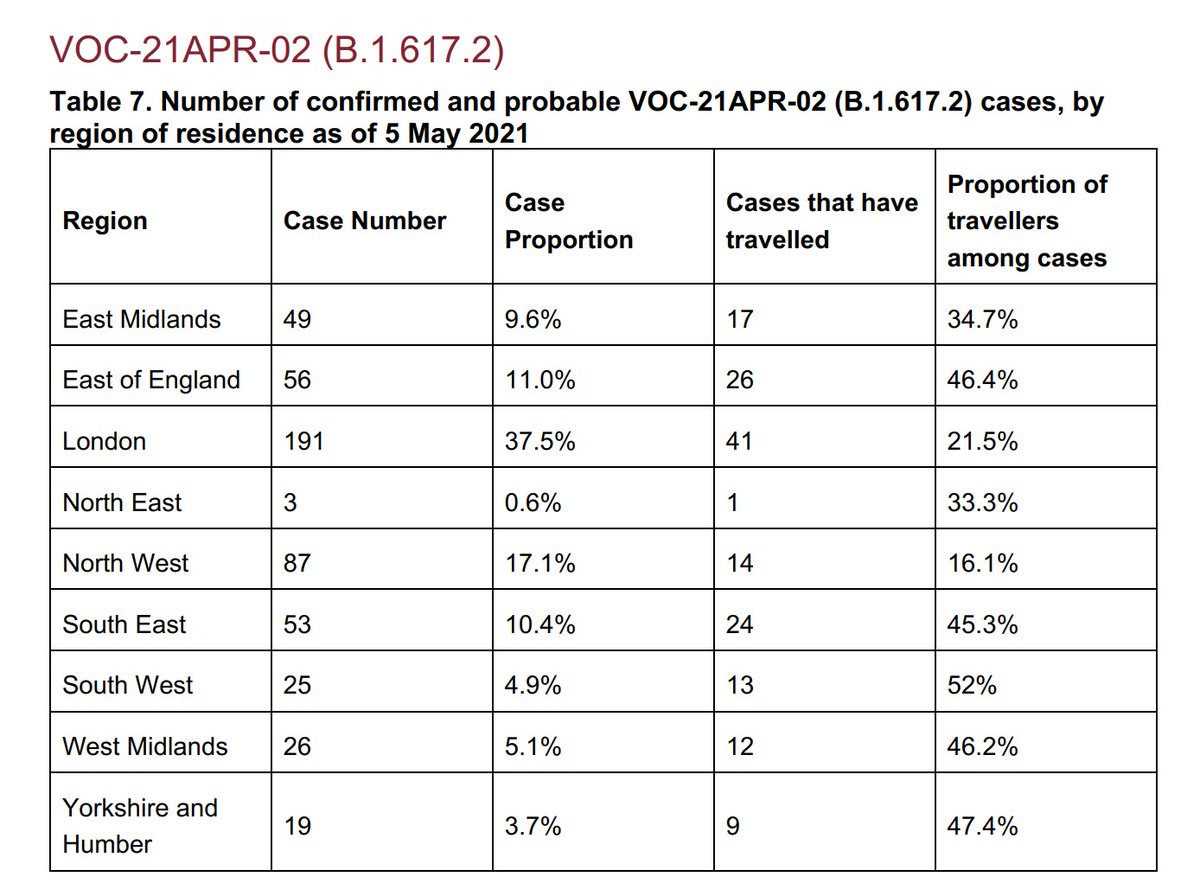
It suggests a *whopping* 37% of sequenced cases in London might be B.1.617.2!
And only 21.5% of cases in London have travelled.
Higher in E Mids, East of England, SE but still less than half. Only 16% of NW cases have travelled (& higher abs numbers).
It's in the community.
And only 21.5% of cases in London have travelled.
Higher in E Mids, East of England, SE but still less than half. Only 16% of NW cases have travelled (& higher abs numbers).
It's in the community.
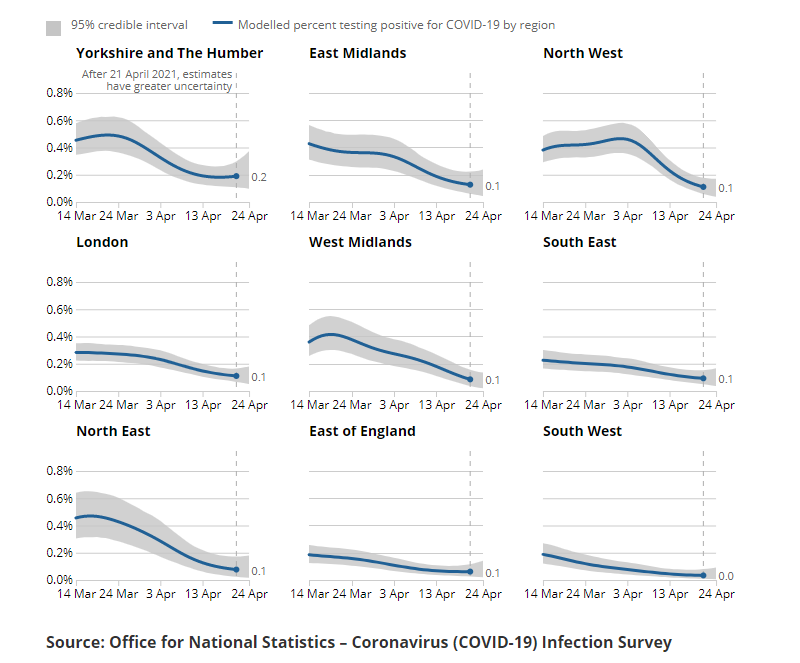
Now these overall sequenced cases are still *low* numbers. So PHE suggest a good proxy for VOC is looking at *all* PCR tests that detect the "S-Gene" (the opposite of how they tracked Kent in winter!). This lets you look at most pillar 2 (community) PCR cases.
This shows London is at almost 50% non B117 (ie NOT "Kent") - and potentially this is all B.1.617.2.
NW also much higher at 30% and East of England above 20%. Perhaps why PHE highlighted NW as of particular concern.
NW also much higher at 30% and East of England above 20%. Perhaps why PHE highlighted NW as of particular concern.
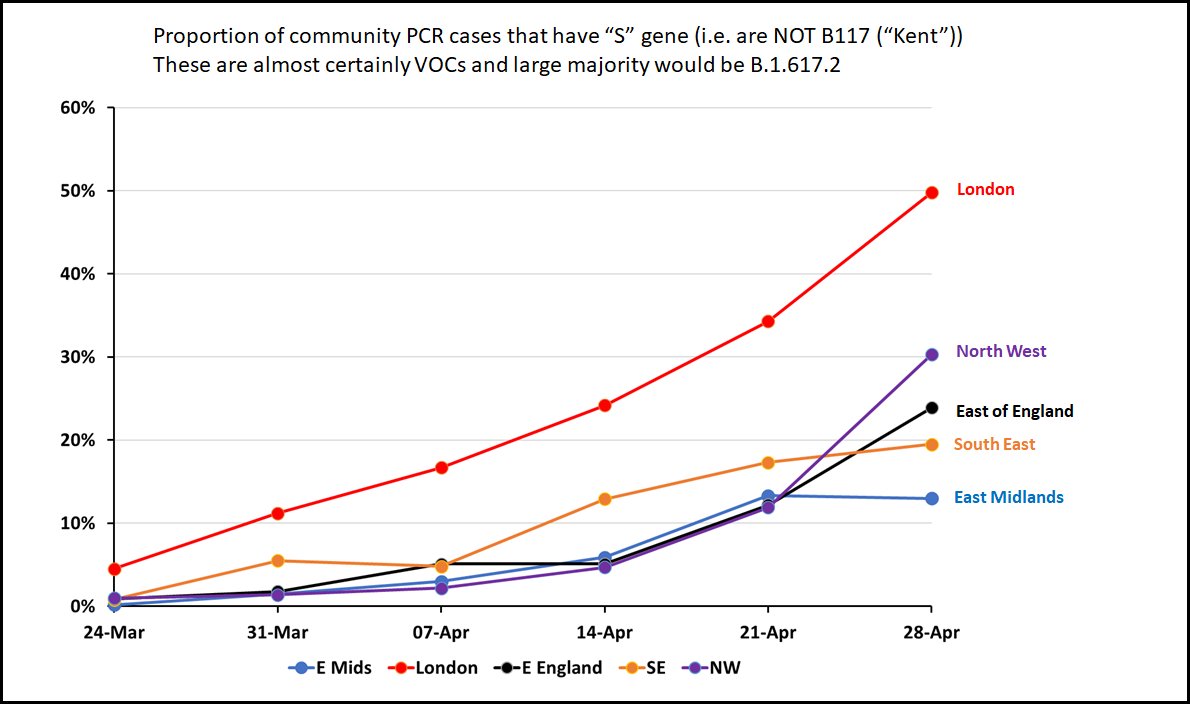
In fact PHE say, that from this way of tracking VOCs, "In some regions... [B.1.617.2] may have replaced B.1.1.7 ["Kent"] to some extent" - i.e. is close to dominant in London (!) (this is page 8, bottom of RH column).
That said, cases in London still v low and flat. *If* this is the case, we might expect cases to rise in London over next few weeks if B.1.617.2 takes over. ONS did say couldn't tell if London had stopped falling this week.
For NW, cases *did* trickle up over last week...
For NW, cases *did* trickle up over last week...
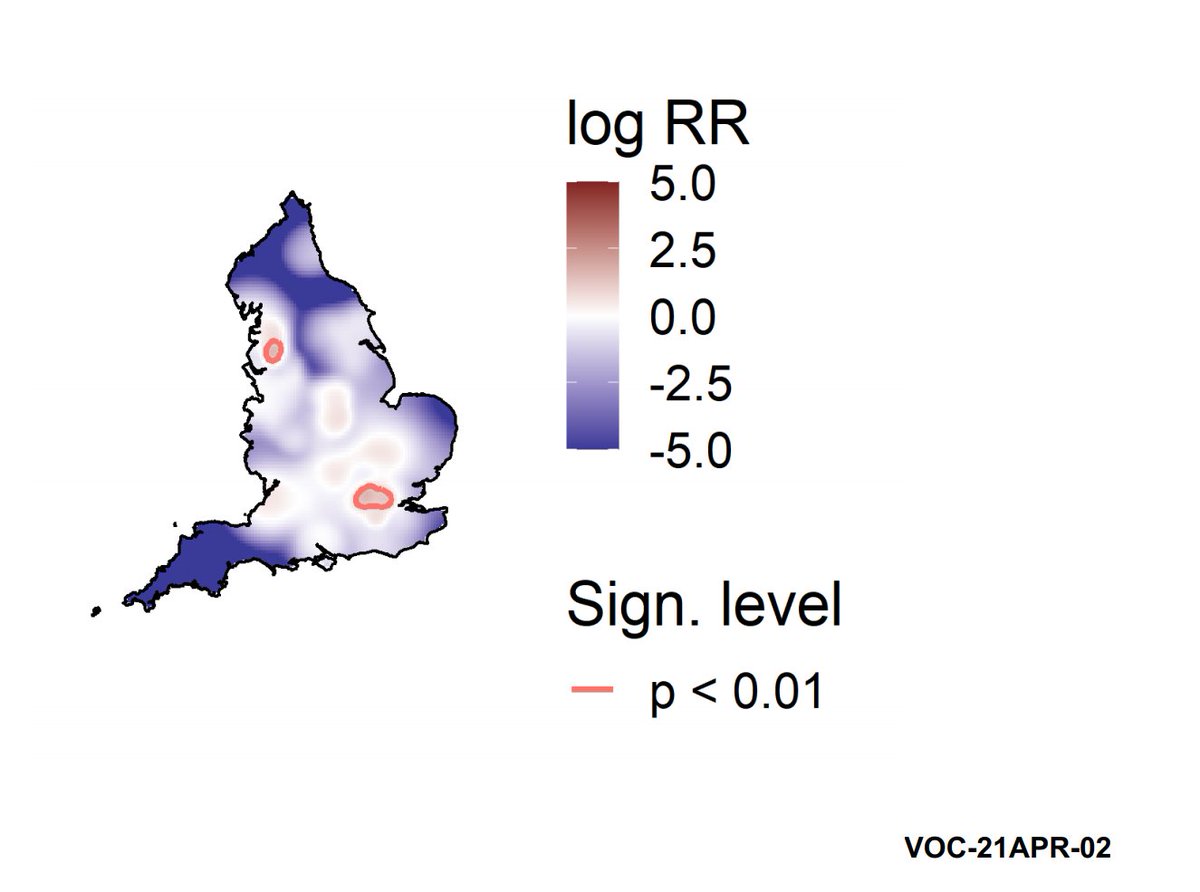
Finally PHE show this map where they think B.1.617.2 is concentrated - blue is almost none, white is some, pinker is more.
Cases concentrated in London and NW (circles), but also spread around Midlands, SE.
Cases concentrated in London and NW (circles), but also spread around Midlands, SE.
So all in all quite a concerning report. Note that out of 507 confirmed B.1.617.2 only 38% were in travellers or contacts of travellers (fig 12 data). The rest were not travel assoc. or unknown - as I said above, it's in the community. It's partly why PHE so worried.
Some people point to low overall case numbers and say some of this could just be an artefact of imported cases doing a bit of spread. And I'd say maybe EXCEPT that we've watched it spread through India where low cases are NOT the issue. And it's outcompeting B117 there.
There's lots we don't know yet.
But even in best case where vaccines work as well against it as they do against B117 ("Kent"), more infectiousness could cause a nasty summer wave just through high numbers.
But even in best case where vaccines work as well against it as they do against B117 ("Kent"), more infectiousness could cause a nasty summer wave just through high numbers.
Hopefully now that PHE have designated VOC, we will get more info on outbreaks and the greater resources can try to contain it.
Seeing how this growth interacts with 17th May opening & highish vax will be a crunch point.
Fingers crossed. /END
Seeing how this growth interacts with 17th May opening & highish vax will be a crunch point.
Fingers crossed. /END
PS I will add that this does not mean we could end up in India's situation - our high vax rates will help even if there were some immune escape (of which there is so far little evidence in any case). But it's still not great.
• • •
Missing some Tweet in this thread? You can try to
force a refresh