Why am I now opposed to any further AstraZeneca vaccine being used in Canada? I want to walk you through the math we have available.
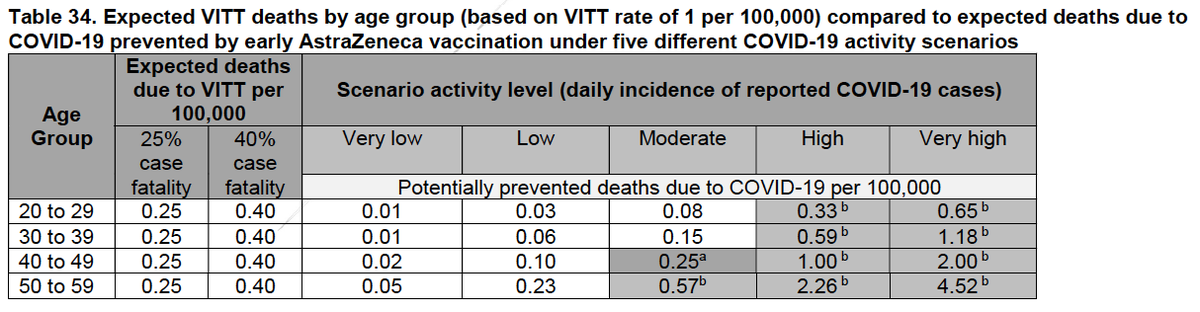
First, I am using some risk-benefit analyses used by @GovCanHealth in their NACI's most recent guidance document.canada.ca/content/dam/ph…
First, I am using some risk-benefit analyses used by @GovCanHealth in their NACI's most recent guidance document.canada.ca/content/dam/ph…


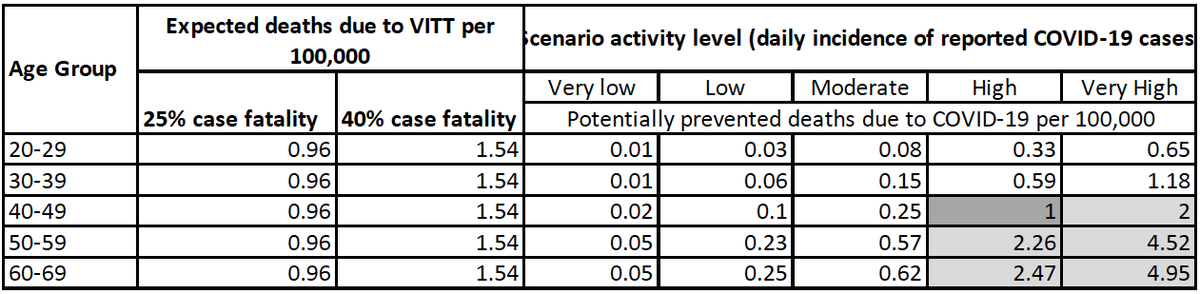
It all hinges on the estimates of VITT. Yesterday @COVIDSciOntario posted a VITT brief covid19-sciencetable.ca/sciencebrief/v… that gave updated estimates of risk: 1:26 000 to 1:127 000 (as opposed to govt doc using 1:100-250K), and I believe ours is the most accurate estimate of risk of VITT.
If we use the revised numbers, the incidence of an ICU admission from AZ vaccine becomes anywhere from 1.27-3.85/100 000. Using existing risk-benefit analysis, it means that it never makes "statistical sense" to use an AZ vaccine where the COVID incidence is moderate (7.5/100K/d)
It also means that AZ makes sense for ages 40-60 if the incidence is high (i.e. 30/100K/d). Where in Canada does that occur? North & South AB, Calgary, Edmonton, Peel, Toronto, and maybe Winnipeg. We should be getting +++ mRNA vaccines to these places ASAP.

Everywhere else, it no longer makes sense based on what we know, to give AZ vaccine.
If we cannot get mRNA vaccine to those other places then, yes, AZ makes sense. AZ made sense in other places a few weeks ago, when the wait for mRNA was longer and the incidence was higher.
If we cannot get mRNA vaccine to those other places then, yes, AZ makes sense. AZ made sense in other places a few weeks ago, when the wait for mRNA was longer and the incidence was higher.
This is my opinion based on the numbers: that we should stop administering AZ vaccine b/c of safety not efficacy. We are lucky, there is tons of mRNA now.
I am certain others will disagree, and I'm ok with that. I'm just trying to inform. But this is what we know today.
I am certain others will disagree, and I'm ok with that. I'm just trying to inform. But this is what we know today.
• • •
Missing some Tweet in this thread? You can try to
force a refresh