
LONG THREAD on B.1.617.2 & latest PHE data covering:
1) latest tech report on B.1.617.2 (aka "India" variant)
2) vaccine efficacy against B.1.617.2
3) consequences for roadmap
4) avoidability... or not.
1) latest tech report on B.1.617.2 (aka "India" variant)
2) vaccine efficacy against B.1.617.2
3) consequences for roadmap
4) avoidability... or not.
2. So first off, PHE tech report released late last night.
Can detect B.1.617.2 by direct sequencing OR by using "S gene" in a PCR test (now 99% of these are B.1.617).
BOTH these methods now estimate that as of 15th May B.1.617.2 was on cusp of being dominant English variant.
Can detect B.1.617.2 by direct sequencing OR by using "S gene" in a PCR test (now 99% of these are B.1.617).
BOTH these methods now estimate that as of 15th May B.1.617.2 was on cusp of being dominant English variant.


3. There is no evidence that B.1.617.2 causes more severe illness than B.1.1.7 (aka "Kent" variant). This is good news but data still quite sparse.
4. The estimated growth advantage of B.1.617.2 (new variant) over B.1.1.7 ("Kent") is 99% per week - ie it is growing twice as fast.
No other variant even comes close.
No other variant even comes close.

5. Now for "secondary attack rates" - how likely a close contact of a confirmed infected person is to get infected themselves.
The *only* variant so far which has shown a significantly higher attack rate than B.1.1.7 ("Kent") is B.1.617.2 - and it's about 50% higher.
The *only* variant so far which has shown a significantly higher attack rate than B.1.1.7 ("Kent") is B.1.617.2 - and it's about 50% higher.
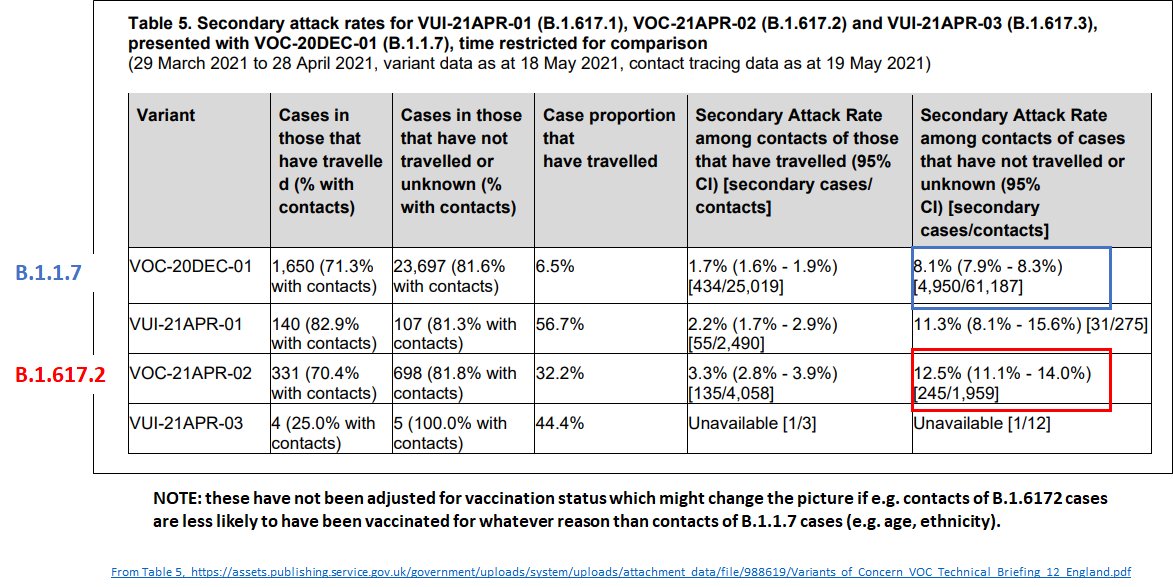
6. Now this has *not* been corrected for vaccination status - if contacts of B.1.617.2 cases are less likely to be vaxxed than those of B.1.1.7 cases this could distort the picture.
But certainly it's v likely that B.1.617.2 does have a higher attack rate, even if less than 50%
But certainly it's v likely that B.1.617.2 does have a higher attack rate, even if less than 50%
7. Where is it? Growing fastest in NW & East of England. Definitely dominant in NW of England (~70% of cases), probably dominant in London, SE, SW.
Low but growing in Yorks & Midlands.
Low but growing in Yorks & Midlands.
8. Note: SW has v few cases and most of its B.1.617.2 cases are travellers so take those numbers with a pinch of salt.
But elsewhere cases of travellers are a minority and only 2.5% in NW.
But elsewhere cases of travellers are a minority and only 2.5% in NW.

9. The only good news here is that despite being likely dominant, London growth of B.1.617.2 has been much flatter for past 2 weeks and cases not gone up much.
This might be a sign that B.1.617.2 is not as scary as it seems - but it's one of the few signs.
This might be a sign that B.1.617.2 is not as scary as it seems - but it's one of the few signs.

10. The other *potentially* good sign is that there *are* some local authorities where B.1.617.2 is dominant but cases remain low.
BUT all the Local authorities with v high case rates have B.1.617.2 dominant. So - complex picture.
BUT all the Local authorities with v high case rates have B.1.617.2 dominant. So - complex picture.

11. Nonetheless, even in slowest growth area of London, "S gene" cases (ie mainly B.1.617.2) are doubling every 2 weeks.
In other regions doubling times are 4-9 days. This is *fast*.
In other regions doubling times are 4-9 days. This is *fast*.
12. Not all of that growth is because more transmissibility - there are context dependent factors, some chance, low background rates that complicate things.
BUT PHE conclude that *some* growth is because more transmissible than B.1.1.7.
BUT PHE conclude that *some* growth is because more transmissible than B.1.1.7.

13. This brings PHE into line with SAGE minutes from 13th May where they say highly likely to be more transmissible and realistic scenario that it's 50% more transmissible.
assets.publishing.service.gov.uk/government/upl…
assets.publishing.service.gov.uk/government/upl…
14. Now... what about vaccines?! Last night, PHE also released a report about real world effectiveness of vaccines vs B.1.617.2.
It's been widely billed as a good news story. I don't think it is really. (did a long thread yesterday:
It's been widely billed as a good news story. I don't think it is really. (did a long thread yesterday:
https://twitter.com/chrischirp/status/1396154081106874382?s=20)
15. The remarkable thing is that even PHE don't think it's good news - they *updated* their risk assessment yesterday for vaccine escape from AMBER to RED.
PHE think this study on vax effectiveness has made B.1.617.2 a *greater* risk.
PHE think this study on vax effectiveness has made B.1.617.2 a *greater* risk.

16. Essentially - YES two doses work almost as well against B.1.617.2 as they do against B.1.1.7.
And in a country that had 3 weeks between doses, this would be less of an issue.
But we are not that country.
And in a country that had 3 weeks between doses, this would be less of an issue.
But we are not that country.
17. We are doing 10-12 weeks between doses - now being reduced to 8 weeks for over 50s.
In the context of a rapidly growing variant against which vax is only 33% after 1 dose, 8 weeks is a LONG time.
In the context of a rapidly growing variant against which vax is only 33% after 1 dose, 8 weeks is a LONG time.
18. Added to that - PHE reported AZ vaccine as only 60% effective for symptomatic infection against B.1.617.2 two weeks after 2nd dose (compared to 66% against B.1.1.7)
khub.net/documents/1359…
khub.net/documents/1359…

19. Which is considerably lower than was reported for AZ in PHE vaccine efficacy update for B.1.1.7 on 16th May where it was given as 85-90%!

20. Now PHE explain that this is because it takes longer for AZ to build up immunity after each dose - so after 4 or 5 weeks likely to go over 80%.
Which is great - except when you have a variant doubling every week.
Which is great - except when you have a variant doubling every week.
21. We currently have 43% of adults who have received 2 doses of vaccine. Only 33% of those are 2 weeks out from their 2nd dose.
Adding in kids, and it's only 30% of population who are fully vaccinated.
Adding in kids, and it's only 30% of population who are fully vaccinated.
22. Given this new variant, this is not high enough. We are a few months away from offering 2nd dose to all adults (August if we can accelerate timetable, Sept if we can't).
Once large majority of adults FULLY vaccinated, in much better position.
Once large majority of adults FULLY vaccinated, in much better position.
23. And it's what happens in the meantime that is worrying me.
SAGE models from 5th May show that a variant that is 40%-50% more transmissible than B.1.1.7 ("Kent") with NO vax escape can strain hospitals as badly as January.
assets.publishing.service.gov.uk/government/upl…
SAGE models from 5th May show that a variant that is 40%-50% more transmissible than B.1.1.7 ("Kent") with NO vax escape can strain hospitals as badly as January.
assets.publishing.service.gov.uk/government/upl…

24. SAGE consensus statment 12 May show they remain worried about this - and that while surge vax is unalloyed good, it is not enough on its own.
assets.publishing.service.gov.uk/government/upl…
SAGE minutes 13 May highlight "earlier, harder, broader" measures to tackle spread.
assets.publishing.service.gov.uk/government/upl…
assets.publishing.service.gov.uk/government/upl…
SAGE minutes 13 May highlight "earlier, harder, broader" measures to tackle spread.
assets.publishing.service.gov.uk/government/upl…


25. JUNIPER group for SAGE 13 May are clear that:
"In the face of uncertain evidence the risk of over-reacting seems small compared to the potential benefit of delaying a third wave until more people are vaccinated"
assets.publishing.service.gov.uk/government/upl…
TBC
"In the face of uncertain evidence the risk of over-reacting seems small compared to the potential benefit of delaying a third wave until more people are vaccinated"
assets.publishing.service.gov.uk/government/upl…
TBC

26. But people have been saying we've not seeing big increases in overall numbers of cases.
But that's cos we've had 2 epidemics - 1 declining (B.1.1.7) and 1 growing (B.1.617.2). While B.1.1.7 remained dominant, it masked the growth of B.1.617.2 and kept case numbers down.
But that's cos we've had 2 epidemics - 1 declining (B.1.1.7) and 1 growing (B.1.617.2). While B.1.1.7 remained dominant, it masked the growth of B.1.617.2 and kept case numbers down.

27. Once B.1.617.2 (about now), this will shift - assuming it keeps growing.
As it happens, cases in England increased by 10% this past week.
As it happens, cases in England increased by 10% this past week.
28. ALL of the B.1.617.2 growth in the data so far is under STEP 2 of the roadmap - i.e. before 17th May.
The additional impact of Monday's opening will become clear over next few weeks. SAGE obv worried in their docs from 13th May.
The additional impact of Monday's opening will become clear over next few weeks. SAGE obv worried in their docs from 13th May.
29. The data do NOT support moving to step 4 of the roadmap unless the current risk assessment of B.1.617.2 reduces significantly.

30. Right now, we should reintroduce masks in schools, accelerate vax and make vax more accessible to communities, support people to isolate and support businesses & schools to improve ventilation.
31. If B.1.617.2 does not start looking less scary, we must wait until we have fully vaxxed more people.
IF cases keep going up next week - consistent with continued rapid growth of B.1.617.2 - we should consider rolling back step 3 of roadmap.
IF cases keep going up next week - consistent with continued rapid growth of B.1.617.2 - we should consider rolling back step 3 of roadmap.
32. Allowing cases to keep going up results in a lot more long covid, risks SAGE predictions becoming true for Jan level surge, & risks further evolution of variant.
33. Waiting too long as we did in March, September & December means that restrictions if they do come will be longer and harsher.
We don't want to do that AGAIN.
As JUNIPER said for SAGE:
"Incontrovertible evidence that B.1.617.2 is more transmissible may come too late"
We don't want to do that AGAIN.
As JUNIPER said for SAGE:
"Incontrovertible evidence that B.1.617.2 is more transmissible may come too late"
34. FINALLY - this was not inevitable. Many have written about delay of red list status for India & our leaky borders.
politics.co.uk/week-in-review…
Yesterday's PHE report shows big reduction in traveller cases a few days post red list. What if we *had* done it weeks earlier? /END
politics.co.uk/week-in-review…
Yesterday's PHE report shows big reduction in traveller cases a few days post red list. What if we *had* done it weeks earlier? /END

35. PS: Now that B.1.617.2 likely dominant, we've lost the initial containment battle. Now it's a race between full vaccination & the variant. And we have to hope that its transmissibilty is limited.
Additional measures (like isolation) help us, opening further helps it.
Additional measures (like isolation) help us, opening further helps it.
36. PPS. More on avoidability. Watch how B.1.617.2 has taken over past month, the change in PHE language (to more concern) & wonder: what if we'd intervened back at end of April when already doubling weekly?
Oh and: what exactly made opening on 17th May seem like a good idea?
Oh and: what exactly made opening on 17th May seem like a good idea?

• • •
Missing some Tweet in this thread? You can try to
force a refresh










