
What do we known about ORIENT GENE used in the Daily Contact Testing Trial by the @educationgovuk and @DHSCgovuk?
There have been claims that this test is as good as others and has been reviewed by @MHRAgovuk for use in assisted testing. This is not right
1/10
There have been claims that this test is as good as others and has been reviewed by @MHRAgovuk for use in assisted testing. This is not right
1/10
The process does not make sense.
The MHRA never review products for assisted testing as they are professional use tests, which go through the self-certification process to get a CE-IVD mark.
MHRA doesn't go near this process.
2/n
The MHRA never review products for assisted testing as they are professional use tests, which go through the self-certification process to get a CE-IVD mark.
MHRA doesn't go near this process.
2/n
In fact ORIENT GENE is not even on the MHRA register of products which is a requirement. You can check here - both for the product and manufacturer (sorry for the messy link).
3/n
aic.mhra.gov.uk/era/pdr.nsf/na…
3/n
aic.mhra.gov.uk/era/pdr.nsf/na…
There are two sets of data on ORIENT GENE we can find in the world's literature. Both are in the Porton Down report here
thelancet.com/journals/eclin…
4/n
thelancet.com/journals/eclin…
4/n
The Phase 3a study was an analytical valdiity type study testing viral transport media (not swabs) from biobanked samples from the Oxford hospital (presume from patients but detail not given). This is not an assessment of using test according to manufacturers instructions.
5/n
5/n
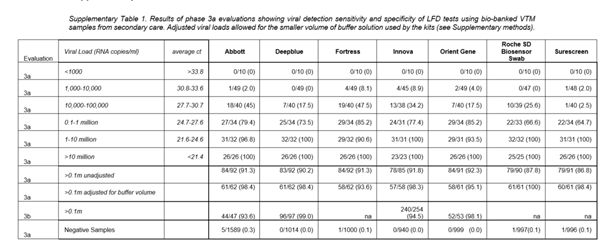
The Phase 3b study used swabs from people with symptoms at test-and-trace centres. The 95 samples were tested by scientists at Porton Down. This sample size is pretty small to assess comparability.
6/n
6/n

There are no data from using the test
(a) by non-scientific experts
(b) in people without symptoms
(c) in children
All of which we would expect to lead to lower sensitivity
7/n
(a) by non-scientific experts
(b) in people without symptoms
(c) in children
All of which we would expect to lead to lower sensitivity
7/n
The MHRA Target Product Profile for using tests to rule infection states data from 150 cases from the real world setting need to be assessed with a sensitivity of 97%. These data do not get close to this.
8/10
8/10
It is not clear to me how the Daily Contact Tracing Trial will estiamte the accuracy of Orient Gene. There was no component in the protocol to do this, and there is no scheduled double testing with Orient Gene and PCR at the same time
9/10
9/10
The summary information sheets from the trial do not provide any summary of the data supporting Orient Gene and this seems a pretty weak basis for using a test in 1000s of children. This is why I have concerns with this test being used in this trial.
10/10
10/10
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh












