
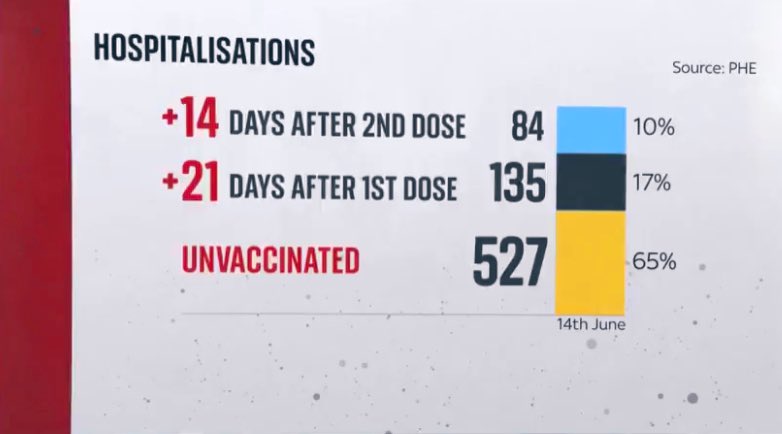
10% of all #COVID19 hospitalizations last week were among fully vaccinated, despite >50% adults fully vaccinated in the UK— ➡️ this is the #DeltaVariant, which is 99% of all 🇬🇧 cases. I’m a big 2-dose vaccine advocate—but we still need strong precaution.🧵news.sky.com/story/covid-19… 
2) Please take #DeltaVariant seriously — it’s the fastest transmission variant known to date. Much much faster. And it has somewhat vaccine evasion, especially 1 dose, and it is much more severe (higher risk of hospitalization)
https://twitter.com/DrEricDing/status/1405633531695489027
3) Because #DeltaVariant is roughly 2x more contagious — ie 2x the R0 of the original virus, the R0 of Delta is likely 6-7. Let’s assume 6, and someday hit 70% *2-dose* with 90% efficacy (but AZ is ~60%), only then can we stop it… but no country is there yet.
HT @GosiaGasperoPhD
HT @GosiaGasperoPhD

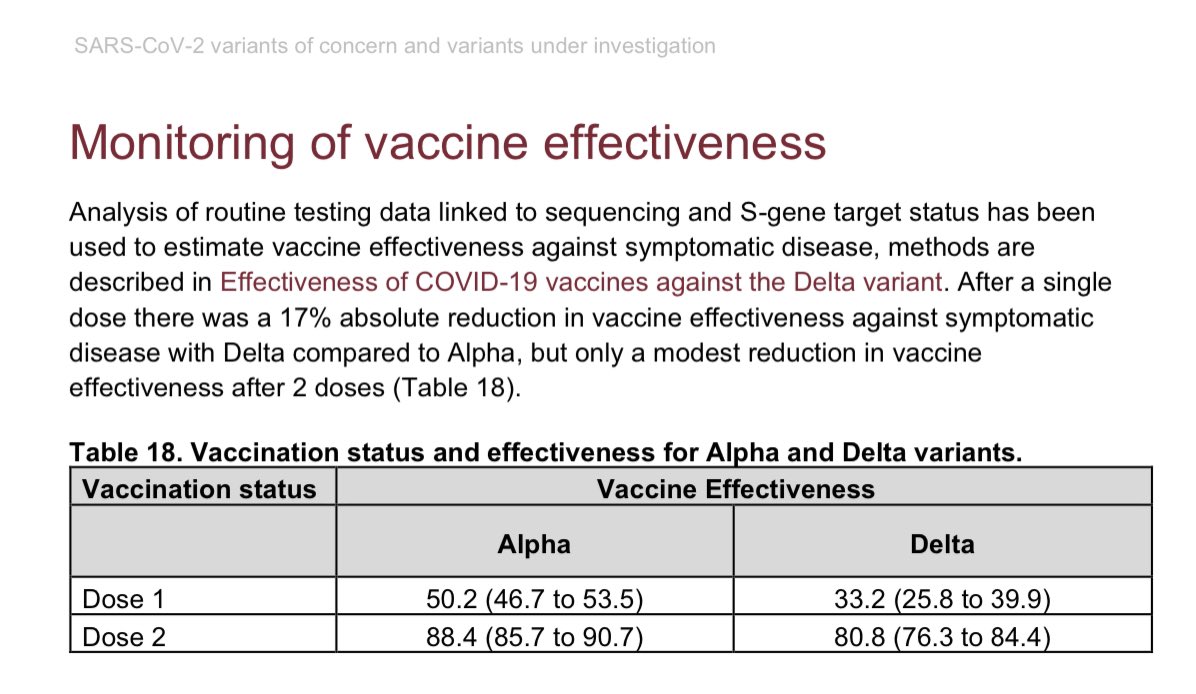
4) But efficacy of AZ against #DeltaVariant is not 90% (it’s 60%), Pfizer is 88% in one non-trial study. However, 1 dose of vaccine (both types averaged) is just 33%. And many countries are just 1 dose vaccinated.
https://twitter.com/drericding/status/1396332689955950594
5) Even @JoeBiden is warning everyone about #DeltaVariant and the urgency to get 2 dose vaccinated. And that it’s dangerous to young people. That’s quite a statement of a presidential warning.
https://twitter.com/DrEricDing/status/1406203178870247433
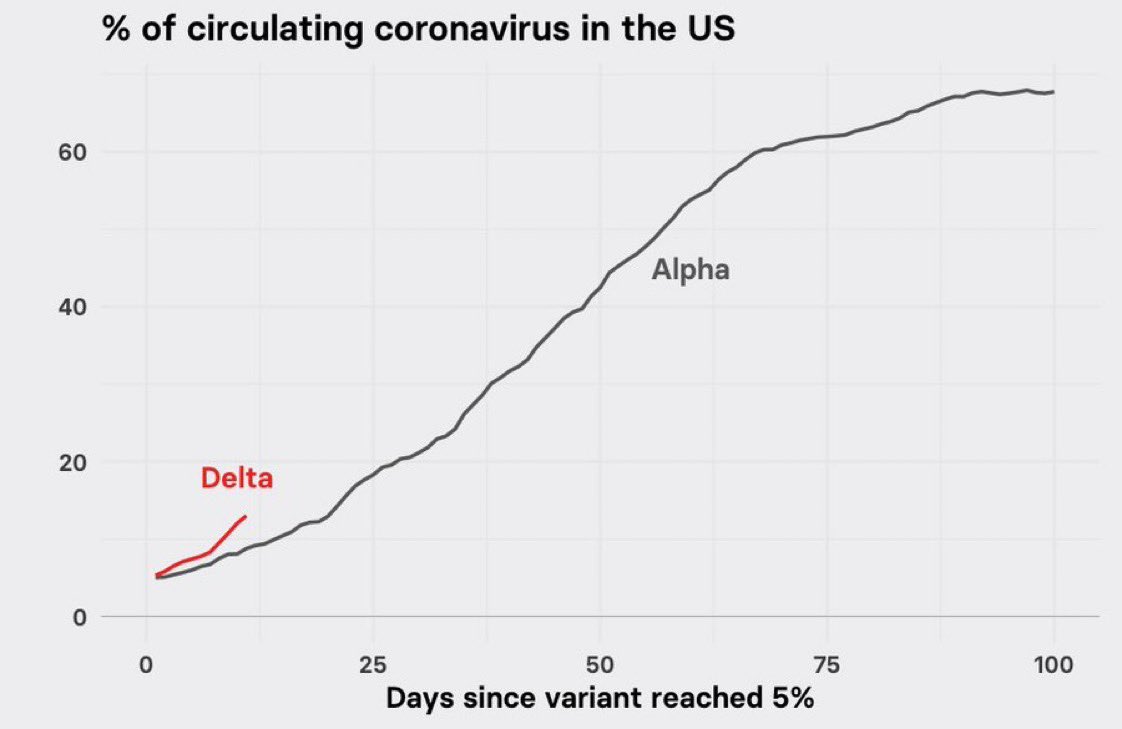
6) Look at the trajectory of Delta versus the previous reigning #alphavariant - former most common variant worldwide. Delta is spreading much faster in the US (and in UK too - where it’s now 99%)
7) Aside from New England, most of the US is not higher in fully vaccinated than UK 🇬🇧. And the Deep South and certain Mountain zone states very low vaccination rate. This bodes poorly for when #DeltaVariant surges more. And it will.

8) last week, CDC finally upgraded #DeltaVariant warning to VOC. But the WHO warned and upgraded Delta being a VOC back in early Many. Over 4 weeks ago!
This is CDC’s biggest fumble of the year. Now #Delta is over 10% of all cases in US and surging.
This is CDC’s biggest fumble of the year. Now #Delta is over 10% of all cases in US and surging.
https://twitter.com/DrEricDing/status/1404847230205505550
9) This is the Delta variant causing double outbreaks in 2 schools in Israel 🇮🇱 this week alone.
https://twitter.com/drericding/status/1406441282860429315
10) if you watch one short video series today, let it be this one on the #DeltaVariant - this is why we need to be vigilant. Part 1 of 3. See thread 🧵for rest of the series… ⬇️
https://twitter.com/drericding/status/1403132149243461635
11) Not just hospitalizations, but a lot of breakthroughs leading to deaths with #DeltaVariant as well. This is from a PHE 🏴 report last week.
https://twitter.com/drericding/status/1403484668528369664
12) here is another way to look at the #DeltaVariant breakthroughs. This is the same PHE (England’s CDC) data as above but in figure form. Sobering.
https://twitter.com/drericding/status/1404379339144245253
13) Vaccine effectiveness against #DeltaVariant according to @PHE_uk — averaging AstraZeneca & Pfizer together (even if different), you can see a substantial drop for 1 dose. But even 2 doses has a ~8% drop as well. Also AZ’s 2 dose is actually 60%.
assets.publishing.service.gov.uk/government/upl…
assets.publishing.service.gov.uk/government/upl…
14) Someone in every state and local govt needs to see the data and hear the warning that #DeltaVariant is coming. We all want the damn pandemic to be over, but we were just in an intermission. Act 2 is coming. India 🇮🇳 was the warning to the world what #B16172 Delta could do. ⬇️
https://twitter.com/DrEricDing/status/1406681179219189760
15) The CDC needs to take urgent action now. endcoronavirus.org/blog/cdc-unive…
16) Siri, define “#DeltaVariant is fast spreading”….
➡️ Delta variant can infect people in mere seconds via fleeting contact.
Siri, does this fleeting exposure infection happened often?
➡️ it happened twice in one outbreak. Video camera evidence supported. See thread 🧵 ⬇️
➡️ Delta variant can infect people in mere seconds via fleeting contact.
Siri, does this fleeting exposure infection happened often?
➡️ it happened twice in one outbreak. Video camera evidence supported. See thread 🧵 ⬇️
https://twitter.com/DrEricDing/status/1406779894785351688
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















