
New outbreak in 44 kids at a middle school in Israel 🇮🇱 with #DeltaVariant, the second such outbreak at a school this week—both Delta. Several fully vaccinated adults also infected at school. 🇮🇱 also recently stop requiring #COVID19 tests upon arrival. 🧵
timesofisrael.com/in-2nd-israeli…
timesofisrael.com/in-2nd-israeli…

2) Israel just approved vaccines for kids 12-15 in early June so kids under 16 haven’t been fully vaccinated yet. But even if fully vaccinated, while lower risk, #DeltaVariant is still problematic.
https://twitter.com/DrEricDing/status/1406421721717030916
3) for those who try to say / claim that kids don’t get sick… 1% hospitalization among kids in UK during #DeltaVariant era is too damn high. Would you roll the dice with 1% hospitalization risk for your kids?
https://twitter.com/jneill/status/1401860709538013186
4) Majority of cases in a large outbreak in an Ontario 🇨🇦 First Nation tribe also in kids. A child is also hospitalized.
https://twitter.com/DrEricDing/status/1405261732994555905
5) Even Joe Biden is warning about the #DeltaVariant and kids. A presidential speech on the topic means it’s a global priority.
https://twitter.com/drericding/status/1406203178870247433
6) do kids transmit? Oh yes. And they have led the infection frontlines in terms of spreading to other age groups.
https://twitter.com/drericding/status/1402056092713168897
7) Take it from Fauci too. Kids transmit and get #LongCovid too. #LongCovidKids
https://twitter.com/drericding/status/1401863233288474630
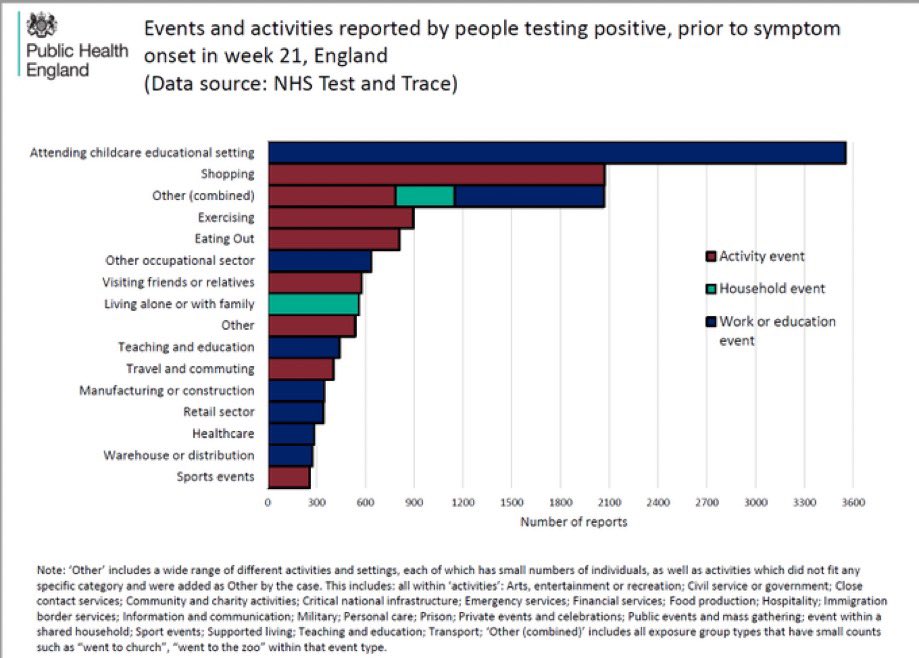
8) Let’s see what UK’s CDC-equivalent PHE found for transmission source during the new surge of #DeltaVariant cases…. Schools. By leaps and bounds.
9) How the hell did we screw up this pediatric Covid thing so badly? Because we didn’t test kids much last year. And variants are much different than old strain. And hence we assumed nothing changed and got complacent.
https://twitter.com/drericding/status/1402058940788228104
10) Delta definitely affects kids a lot. Scores of reports from India as well. See this full video on the #DeltaVariant situation in UK. Part 1 of 3. Other videos in thread 🧵 below.
https://twitter.com/DrEricDing/status/1403132149243461635
11) we should heed what Indian doctors are warning about #DeltaVariant and kids.
https://twitter.com/drericding/status/1403132988255318021
12) Singapore 🇸🇬 Ministry of Health is also warning about #DeltaVariant and kids as well. We need to learn from other countries so that we don’t repeat it ourselves.
https://twitter.com/drericding/status/1394380714041217026
13) More data about #DeltaVariant transmission via schools from recent report on transmission incidents (99% #DeltaVariant in 🇬🇧) in “Educational Settings”. Yes elderly more protected than children, true, but we see a rise in the parent generation of school kids too.

14) this thread 🧵 explains just how fast #DeltaVariant spreads in the real world. Fleeting exposure of mere seconds is all it needs according to very detailed contact tracing in Australia 🇦🇺… and fleeting exposure infection happened twice by one man alone. ⬇️
https://twitter.com/drericding/status/1406779894785351688
15) they have the actual security camera footage of this encounter and infection event. They never actually touched - it was the 2nd fleeting encounter infection from same outbreak. #DeltaVariant is damn infectious.
https://twitter.com/drericding/status/1406784126842245121
16) please sign this petition to CDC for urgent #DeltaVariant action. It is by @endCOVID19 & @CovidActionGrp and a “coalition of scientists, public health officials, epidemiologists, health care workers, educators, advocates, parents, & concerned citizens: change.org/p/centers-for-…
17) Reminder - #LongCovid in kids is real. 1 in 12 kids will develop #LongCovidKids according to UK 🇬🇧 data. Don’t trivialize pediatric cases.
https://twitter.com/drzoehyde/status/1405418023335305216
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















