
It’s interesting I’m being told how long is ideal in #NHS for Clinical Consultations in Outpatients by ‘management’, who can hold as many meetings of undefined purpose and length as they wish at short notice & expect my participation @djnicholl @PeteGordon68 @vincentconnolly
The most important Meetings in #Healthcare are between Patient and Clinician but are not the ones valued and prioritised by management
dropbox.com/s/vd7fybw50ml9…
dropbox.com/s/vd7fybw50ml9…

Imagine if management’s meetings were subject to same rules as outpatients?
Schedule 6 weeks in advance
New Agenda items 30 mins max, Reviews 15 mins. Extra items can be added by anyone but all items must still be discussed. Items for other meetings can be added in Willy Nilly
Schedule 6 weeks in advance
New Agenda items 30 mins max, Reviews 15 mins. Extra items can be added by anyone but all items must still be discussed. Items for other meetings can be added in Willy Nilly
There is to be no preparation for discussion of an agenda item, no papers to be submitted in advance. Key information will be missing. The chair must take all the minutes as well as keep everything on time. The chair must Do all the Actions his/herself. Interruptions encouraged.
The chair may expect to be chairing one set of agenda items but at the start find they have been allocated a random set of items from simultaneous meetings.
I love the idea that management meetings should be scheduled 6 weeks in advance. Then we would know how many meetings and when they were to happen and for how long and maybe even their purpose. I work in an Anarchy of #Teams Meetings now. Is there a structure anymore?
The only way I can both keep my outpatient clinics to time & have satisfactory Consultations is by extensive preparation eg 2hr for a 4hr clinic. But this only works because it’s a solo clinic & patients not swapped between eg Consultant & Registrar to keep to time.
useful idea to think of Clinical Consultation being a serious Meeting of two important people. Both should be briefed, should be an Agenda, secretary to take minutes. No interruptions. Ability to lengthen meeting if necessary. Schedule next meeting etc dropbox.com/s/vd7fybw50ml9…

However busy chaotic and interrupted the Chair must stay calm polite and respectful at all times and take on extra Agenda items with no notice at all, even ones clearly for other meetings. No breaks, no refreshments allowed.
Those #JohnCleese #VideoArts videos on
How not to run meetings
Were possibly based on how ordinary #NHS outpatients and #WardRounds are ‘organised’ and conducted?
How not to run meetings
Were possibly based on how ordinary #NHS outpatients and #WardRounds are ‘organised’ and conducted?
Managers hate being rushed from one late ended meeting to the next with no pause to regroup and refresh mind and body but expect us to relish this in Outpatients and on #WardRounds @j59dd
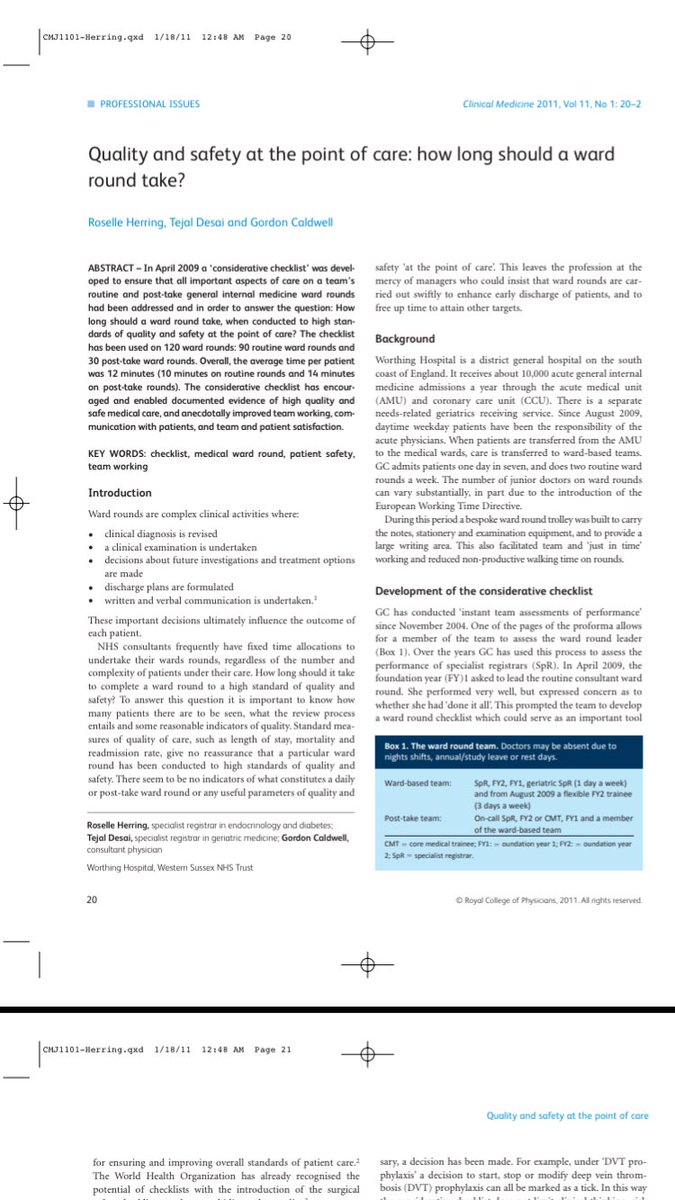
I recall describing #WardRounds as a
Series of Meetings between individual patients and a Clinical Team
#Outpatients are a series of Meetings between individual patients and a clinician
These Meetings should be planned, prepared for and fully supported dropbox.com/s/satkng5d88pb…
Series of Meetings between individual patients and a Clinical Team
#Outpatients are a series of Meetings between individual patients and a clinician
These Meetings should be planned, prepared for and fully supported dropbox.com/s/satkng5d88pb…
Still so common in Outpatients
Your GP asked for us to meet to discuss your health. Did the GP tell you and say why you were to come?
No, I just got an appointment in the post …
Your GP asked for us to meet to discuss your health. Did the GP tell you and say why you were to come?
No, I just got an appointment in the post …
• • •
Missing some Tweet in this thread? You can try to
force a refresh


