Prof Darrel Francis ☺ Mk CardioFellows Great Again
22 Jun,
44 tweets, 9 min read
Ahhhh, interesting that Josh brings this up!
h/t to Sanjay Kaul @kaulcsmc and DJ Cohen @djc795
for highlighting how difficult it is for people to redirect their thinking
h/t to Sanjay Kaul @kaulcsmc and DJ Cohen @djc795
for highlighting how difficult it is for people to redirect their thinking
https://twitter.com/JoshuaBeckmanMD/status/1405368650090045445
What dose of metoprolol do you consider standard?
Here is the UK's British National Formulary (equivalent in role, I believe, to the US Physician's Desk Reference) regarding standard short-acting metoprolol.
Source: bnf.nice.org.uk/drug/metoprolo…
Source: bnf.nice.org.uk/drug/metoprolo…

In particular, for treating the symptom of ischaemia:

Based on the above to snapshots, what would you consider the standard TOTAL DAILY DOSE of immediate-acting metoprolol for management of ischaemia?
Now, we are going to switch to a long-acting alternative, Metoprolol CRXL.
This is not immediate-acting metoprolol.
It is metoprolol attached to some special sciency stuff called CRXL. What does the CRXL stuff do to the metoprolol?
This is not immediate-acting metoprolol.
It is metoprolol attached to some special sciency stuff called CRXL. What does the CRXL stuff do to the metoprolol?
Obviously it slows the release.
Hence the name, slow release. ("Controlled Release, Xtra Long" or whatever it is CRXL stands for)
But the slowing of the releasing also causes some of it never to be released at all into the blood stream.
Hence the name, slow release. ("Controlled Release, Xtra Long" or whatever it is CRXL stands for)
But the slowing of the releasing also causes some of it never to be released at all into the blood stream.
Remember the bioavailability graphs you snored through during Second-Year Pharmacology in Med School?

The slower release tablet has a smaller peak and a longer tail.
But the longer-ness of the tail never quite compensates for the smaller-ness of the peak.
The AREA UNDER CURVE of the slow-release curve is therefore typically ...
But the longer-ness of the tail never quite compensates for the smaller-ness of the peak.
The AREA UNDER CURVE of the slow-release curve is therefore typically ...
How much smaller?
That needs to be measured by experiment.
Like this one shown in sci-hub.cat/10.2165/000030…
That needs to be measured by experiment.
Like this one shown in sci-hub.cat/10.2165/000030…

And here are the numbers from several studies such as the one pictured above, summarised (in the same review article linked to above):

If you had to give a single estimate, based on the above fractions, how would you complete this sentence?
The relative bioavailability of Controlled Release metoprolol, compared with Conventional Tablet metoprolol, is about ...
The relative bioavailability of Controlled Release metoprolol, compared with Conventional Tablet metoprolol, is about ...
So suppose your CONVENTIONAL tablet metoprolol dose was going to be 50mg three-times-a-day, i.e. 150 mg per day,
What should your daily dose of controlled-release metoprolol be, so that 75% of it comes to 150mg?
What should your daily dose of controlled-release metoprolol be, so that 75% of it comes to 150mg?
Right, so let's look at POISE, shall we?


On the day of the operation, what dose of metoprolol CRXL was given BEFORE the op?
What given in the following 6 hours?
What given in the following 6 hours?
So what was the total dose on the DAY OF THE OPERATION (from 4 hours pre, to 6 hours post)
The NEXT DAY, they could have another 200mg, and so on.
So where did the 400mg story come from?
So where did the 400mg story come from?

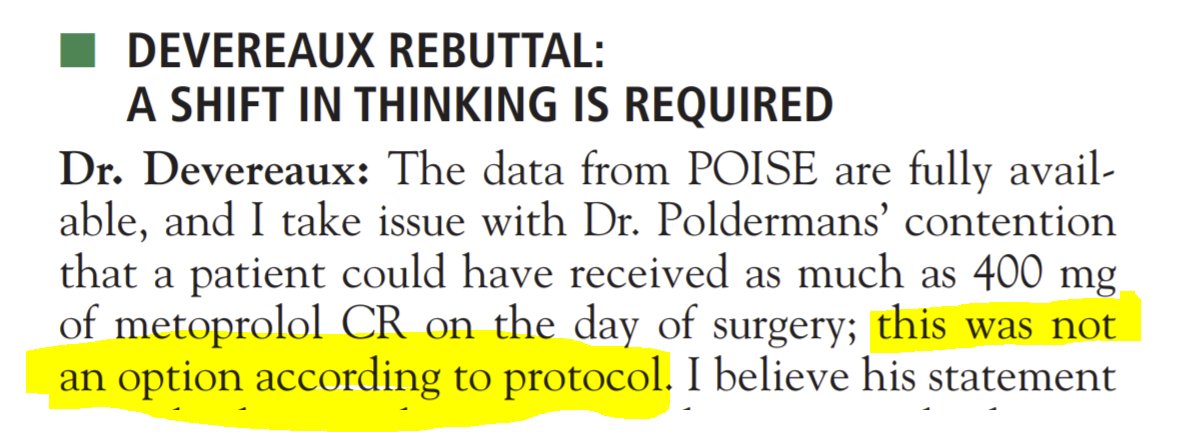
Completely fabricated, in full view of the public, by Uncle Don. (Who would have thought he would make things up, eh?)
And _immediately_ corrected, equally publicly, by the rigorous trialist PJ Devereaux himself.
And _immediately_ corrected, equally publicly, by the rigorous trialist PJ Devereaux himself.
The allegation of POISE using an unusually "high dose of beta-blockers" was later repeated in this article, which was widely read.
I have removed the names of authors because one of them recently initiated a complaint against me to my employer, which the employer upheld.
I have removed the names of authors because one of them recently initiated a complaint against me to my employer, which the employer upheld.
My employer says I must no longer say that the DECREASE trials were made up, because (because of the nature of my employment) people reading my tweet may believe that that is the opinion of Imperial College.
I believe I am free to say the 400mg thing is made up by Don P, because there is evidence in writing. (Although I shall await with trepidation an ominous telephone call.)
And I can show this table which was what Don Poldermans' university found when it looked into his trials:
And I can show this table which was what Don Poldermans' university found when it looked into his trials:


Full story here:
sci-hub.cat/https://doi.or…
(I don't think I can be sacked for citing my own paper. Well, if I can, it would be a fun way to go!)
sci-hub.cat/https://doi.or…
(I don't think I can be sacked for citing my own paper. Well, if I can, it would be a fun way to go!)
And if we recall how we got into this, which was Josh Beckman's tweet:

Yes, certainly don't do what POISE did, but that was only to initiate (what you have all correctly identified to be) perfectly standard doses of beta blockade routinely to at-risk patients.
But it was NOT 400mg.
It was the equivalent of 50mg 3-times a day conventional metoprolol,
namely 200mg CRXL once a day
It was the equivalent of 50mg 3-times a day conventional metoprolol,
namely 200mg CRXL once a day
I was annoyed (like many people were) that NEJM has not retracted DECREASE I. I wrote to them and whinged, and was dissatisfied with their reply.
But then I travelled to USA and ambushed John A Jarcho, Deputy Editor of NEJM:

And I was astonished.
Without any advance notice, and 2 years after receiving the letter, he could recall a great deal of it.
He did not have any objection to our reasoning that what was reported was mathematically impossible.
Without any advance notice, and 2 years after receiving the letter, he could recall a great deal of it.
He did not have any objection to our reasoning that what was reported was mathematically impossible.
His problem was that the journal can only retract a paper if
(a) authors ask for it
or
(b) the authors' institution asks for it
(a) authors ask for it
or
(b) the authors' institution asks for it
I then (finally!) began to have sympathy for the predicament of journal editors.
They are not special stupid people who can't see what you or I can see.
They are just people who have rules to follow.
They are not special stupid people who can't see what you or I can see.
They are just people who have rules to follow.
Just like police who can't arrest Al Capone for being a gangster, because they can't prove it,
editors can't retract papers for being made up, unless the the authors or their institutions ask for it.
editors can't retract papers for being made up, unless the the authors or their institutions ask for it.
So that is why I train all the fellows to decide for themselves how reliable results in papers are.
Do not assume that what is published is generally accepted to be true. It may be generally accepted to be UNTRUE, but the barrier to retraction so high that the paper survives.
Do not assume that what is published is generally accepted to be true. It may be generally accepted to be UNTRUE, but the barrier to retraction so high that the paper survives.
We are very fortunate that Erasmus conducted a thorough investigation of the supposed DECREASE trials.
During the investigation, NEJM could have the "Expression of Concern" on the paper.
During the investigation, NEJM could have the "Expression of Concern" on the paper.
But once the Erasmus investigation was over, NEJM *had* to remove the Expression of Concern: they had no choice.
Because the investigation did not request retraction.
Because the investigation did not request retraction.
Investigations (as I would expect of an investigation of myself!) start from a presumption of innocence and require proof of guilt.
If there is no proof, they cannot declare guilt and demand retraction.
If there is no proof, they cannot declare guilt and demand retraction.
As a researcher, you can always say,
"All the data has vanished"
The University can fire you for saying it has vanished, but can't prove the paper you have written from it is made-up.
So the journal CANNOT retract.
"All the data has vanished"
The University can fire you for saying it has vanished, but can't prove the paper you have written from it is made-up.
So the journal CANNOT retract.
The ones who get caught are the poor guys in basic science, who show raw data figures.
Their photos of gels and cells etc have to come from something, so *IF* the originals are found elsewhere (e.g. in the same or another paper), they are screwed.
Their photos of gels and cells etc have to come from something, so *IF* the originals are found elsewhere (e.g. in the same or another paper), they are screwed.
But a closing thought to cheer up my fellow clinical researchers:
We don't show raw data.
So our papers can always be protected from retraction by the universal ploy:
"Sorry, all the source data has mysteriously disappeared from the offices and computers of all researchers."
We don't show raw data.
So our papers can always be protected from retraction by the universal ploy:
"Sorry, all the source data has mysteriously disappeared from the offices and computers of all researchers."
Sorry, as for whether "DECREASE I is not the only pro evidence," I suggest this image, which separates the DECREASE trials from normal science.
Source: heart.bmj.com/content/heartj…
Source: heart.bmj.com/content/heartj…

• • •
Missing some Tweet in this thread? You can try to
force a refresh