1/
UK: Delta variant:
What can we learn, and what can we not learn, from PHE reports?
About the IFR? flu at most
About vacciine effect on death? nothing
UK: Delta variant:
What can we learn, and what can we not learn, from PHE reports?
About the IFR? flu at most
About vacciine effect on death? nothing

2/
See here IFR=0.1%, 0.3%
Why estimates differ?
Several explanations, but one we’ll need later: risk is not # death/# people. It is # deaths/# person-time.
Need to add up the number of days each person was observed to compute “rate” (epidemiology).
Risk is over people AND time.
See here IFR=0.1%, 0.3%
Why estimates differ?
Several explanations, but one we’ll need later: risk is not # death/# people. It is # deaths/# person-time.
Need to add up the number of days each person was observed to compute “rate” (epidemiology).
Risk is over people AND time.

3/
We don’t have time (days) for all 92,056 cases. We only have it for 11,250 (28 days per person).
Regardless, these are not all cases. By now it’s clear that 80-90% of infections are asymptomatic.
Therefore IFR must be << 0.3%
Flu. Or less.
Delta much less virulent than Alpha
We don’t have time (days) for all 92,056 cases. We only have it for 11,250 (28 days per person).
Regardless, these are not all cases. By now it’s clear that 80-90% of infections are asymptomatic.
Therefore IFR must be << 0.3%
Flu. Or less.
Delta much less virulent than Alpha
4/
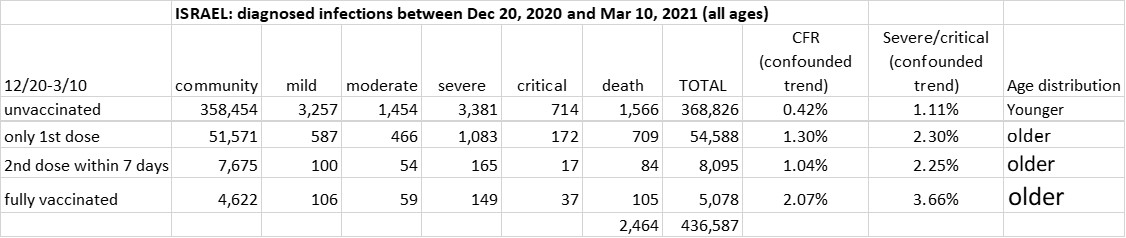
Vacciine effectiveness on death:
Two tables created from June 25 & June 18 reports.
Probability of death in cases is 6-7 times higher in fully vaccinated than in unvaccinated.
That’s not valid inference!
It is not “effect”.
Why?
Vacciine effectiveness on death:
Two tables created from June 25 & June 18 reports.
Probability of death in cases is 6-7 times higher in fully vaccinated than in unvaccinated.
That’s not valid inference!
It is not “effect”.
Why?

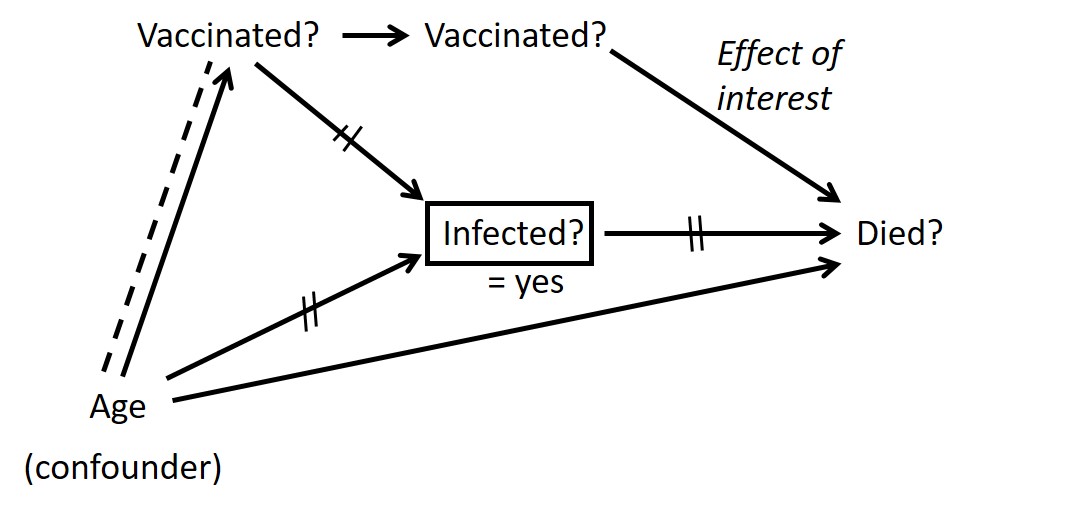
5/
Vaccinated are older than unvaccinated, on average. Older are more likely to die (in general).
That’s called “confounding” (epidemiology).
And age might not be the only confounder.
Vaccinated are older than unvaccinated, on average. Older are more likely to die (in general).
That’s called “confounding” (epidemiology).
And age might not be the only confounder.
6/
How do we de-confound?
One method:
Compare people of the same age (say, “old”).
Can’t compare exactly the same age, so it’s not perfect. But try.
How do we de-confound?
One method:
Compare people of the same age (say, “old”).
Can’t compare exactly the same age, so it’s not perfect. But try.
7/
So, in the last PHE report we have “stratification” for those 3 groups above:
Age <50: 8 deaths
Age 50+: 105 deaths
Inference from 8 deaths? No!
[My rule of thumb: If you can replace cell counts with names, you don’t have data].
So, in the last PHE report we have “stratification” for those 3 groups above:
Age <50: 8 deaths
Age 50+: 105 deaths
Inference from 8 deaths? No!
[My rule of thumb: If you can replace cell counts with names, you don’t have data].
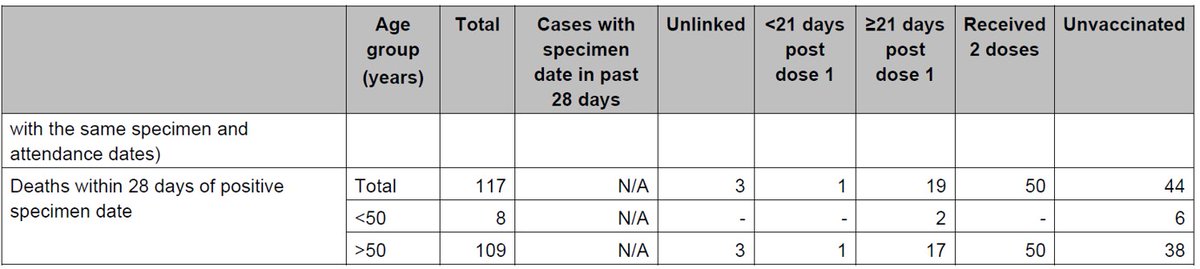
8/
See table for age 50+:
Fully vaccinated worse than partially vaccinated?
Protection by partial vaccination (vs. unvaccinated) stronger than full vaccination?
None of this makes sense.
All comparisons are still severely biased
See table for age 50+:
Fully vaccinated worse than partially vaccinated?
Protection by partial vaccination (vs. unvaccinated) stronger than full vaccination?
None of this makes sense.
All comparisons are still severely biased

9/
Sources of distortion?
1. Need person-time denominator. For example, f/u time likely shorter for Group 2. People move to Group 3 within 2-3 weeks.
2. Group 1 (unvaccinated) much smaller than others.
Sources of distortion?
1. Need person-time denominator. For example, f/u time likely shorter for Group 2. People move to Group 3 within 2-3 weeks.
2. Group 1 (unvaccinated) much smaller than others.
10/
Sources of distortion (cont.)
3. Who are those unvaccinated >50?
Many elderly in compromised health (nursing homes), as suggested by @rzioni ?
Are they comparable to the other groups?
Sources of distortion (cont.)
3. Who are those unvaccinated >50?
Many elderly in compromised health (nursing homes), as suggested by @rzioni ?
Are they comparable to the other groups?
https://twitter.com/rzioni/status/1408472182712324103
11/
As summarized in tweet 1:
IFR: flu at most
Vacciine effect on death: nothing can be inferred
As summarized in tweet 1:
IFR: flu at most
Vacciine effect on death: nothing can be inferred
12/
If spread continues to largely spare the vulnerable (60+), the delta wave in UK (emerging in US, Israel, Sweden,…) is ENDEMIC wave.
Will not cause excess deaths.
Would not have been noticed without extensive monitoring.
If so:
Pandemic phase has ended. Panic has not.
If spread continues to largely spare the vulnerable (60+), the delta wave in UK (emerging in US, Israel, Sweden,…) is ENDEMIC wave.
Will not cause excess deaths.
Would not have been noticed without extensive monitoring.
If so:
Pandemic phase has ended. Panic has not.

*Tweet 2 correction: should be "CFR=0.1%, 0.3%". Not IFR of course.
• • •
Missing some Tweet in this thread? You can try to
force a refresh