1/
Theories & evidence of bias in Israel data on vaccine effectiveness.
nejm.org/doi/full/10.10…
Theories:
1. Important endpoints (hospitalization, severe illness, death) included many patients with incidental positive PCR
2. Preferentially in unvaccinated
Theories & evidence of bias in Israel data on vaccine effectiveness.
nejm.org/doi/full/10.10…
Theories:
1. Important endpoints (hospitalization, severe illness, death) included many patients with incidental positive PCR
2. Preferentially in unvaccinated
2/
All figures taken from Supplementary Appendix Figure S3. (The Y-axis scale seems wrong, but I assume it is just a labeling error)
Key figure: Time to hospitalization
Most patients were hospitalized within 1-2 days (!) of a first PCR swab that was found positive
Unexpected.
All figures taken from Supplementary Appendix Figure S3. (The Y-axis scale seems wrong, but I assume it is just a labeling error)
Key figure: Time to hospitalization
Most patients were hospitalized within 1-2 days (!) of a first PCR swab that was found positive
Unexpected.

3/
Typical course much longer: symptoms->test->worsening symptoms-->hospitalization
What happened?
Many patients were likely tested in the ER. They showed up in severe enough condition, for which no outpatient PCR was done. Thus, their condition on admission was not COVID
Typical course much longer: symptoms->test->worsening symptoms-->hospitalization
What happened?
Many patients were likely tested in the ER. They showed up in severe enough condition, for which no outpatient PCR was done. Thus, their condition on admission was not COVID
4/
Nonetheless, they were hospitalized in Corona wards because they tested positive.
Many were counted as severe COVID cases, and as COVID deaths if they died.
Nonetheless, they were hospitalized in Corona wards because they tested positive.
Many were counted as severe COVID cases, and as COVID deaths if they died.
5/
Other hospitalized patients, PCR-negative on admission, were found positive later. Possibly counted in the first column in the Figure. These might have been infected in the hospital. Hopefully not many.
Other hospitalized patients, PCR-negative on admission, were found positive later. Possibly counted in the first column in the Figure. These might have been infected in the hospital. Hopefully not many.

6/
Note that time to severe disease and time to death are also “condensed” to the left. Does not look like expected spread. Again, I assume just labeling error of the Y-axis.
Note that time to severe disease and time to death are also “condensed” to the left. Does not look like expected spread. Again, I assume just labeling error of the Y-axis.


7/
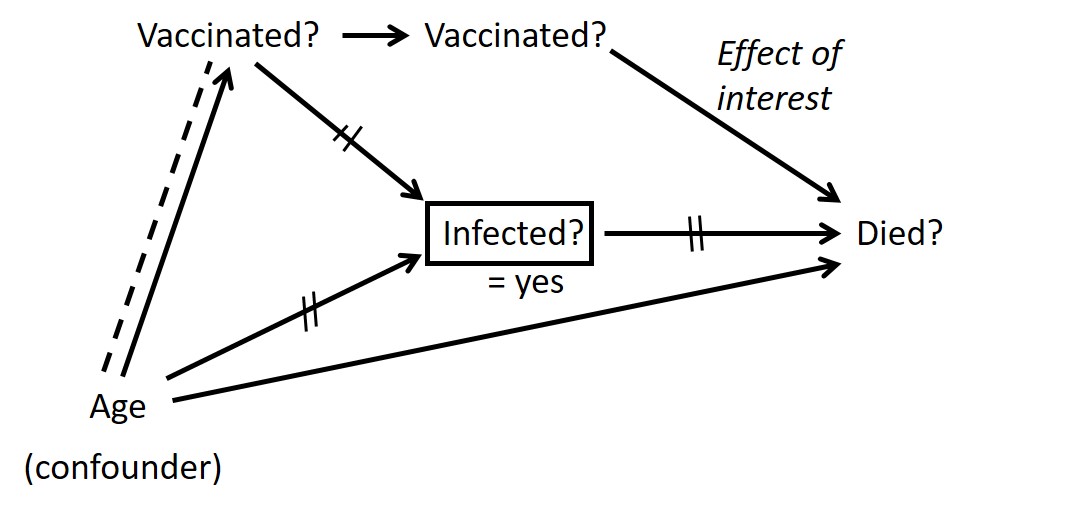
All unvaccinated were tested in the ER. Policy unclear, but at least in some hospitals, vaccinated were tested only if suggestive symptoms.
Thus, endpoint misclassification was differential. Dependent on vaccination status.
All unvaccinated were tested in the ER. Policy unclear, but at least in some hospitals, vaccinated were tested only if suggestive symptoms.
Thus, endpoint misclassification was differential. Dependent on vaccination status.
https://twitter.com/prof_shahar/status/1361749007307997185
8/
Analysis (inspired by an idea of @MatanHolzer) show prolonged, flat death rate in unvaccinated, which is atypical.
Regardless of vaccination, waves usually decline after a fairly short peak.
Analysis (inspired by an idea of @MatanHolzer) show prolonged, flat death rate in unvaccinated, which is atypical.
Regardless of vaccination, waves usually decline after a fairly short peak.

9/
If many deaths in unvaccinated were not COVID-related, prolonged flat death rate may reflect typical death during winter.
If many deaths in unvaccinated were not COVID-related, prolonged flat death rate may reflect typical death during winter.
10/
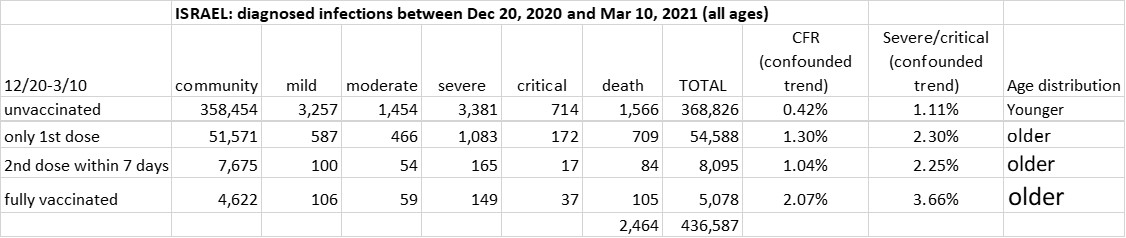
To sum up: Suggestive evidence that non-COVID hospitalizations were counted as COVID. Preferentially in unvaccinated.
Expected result: over-estimation of vaccine effectiveness in Israel data for key endpoints.
To sum up: Suggestive evidence that non-COVID hospitalizations were counted as COVID. Preferentially in unvaccinated.
Expected result: over-estimation of vaccine effectiveness in Israel data for key endpoints.
• • •
Missing some Tweet in this thread? You can try to
force a refresh