
I’m not going to comment on today’s case data, because the message hasn't changed, and I don’t want to spoil an otherwise positive evening. But case data only really matters if it causes bad medical outcomes, and here the news may be a bit better. 1/n
https://twitter.com/JamesWard73/status/1409615627954929672?s=20
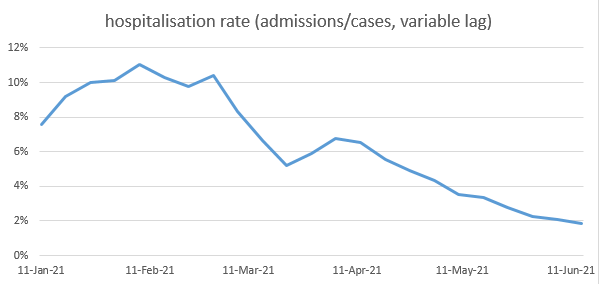
The ratio of hospitalisations to cases has been dropping over the last few months – mostly due to vaccines. (the main effect of vaccines is to stop people getting infected, but for those who do get infected, they also reduce the chances of going to hospital or dying). 2/n 
[note: to calculate this ratio, we need to compare hospitalisations to cases a few days earlier, and there’s some debate as to how long a lag to use. I’ve used lags from this recent ONS study ons.gov.uk/releases/coron…, but I get similar results with different assumptions] 3/n
However, as quite a few people have pointed out (see below), there’s a good chance that this ratio is being distorted by changes in the age-mix of cases: in particular, as cases grow in younger groups, with lower risk, they will pull the ratio down. 4/n
https://twitter.com/DaniAlmazan_/status/1409866141854539778?s=20
So can we work out how much of the fall is due to age-mix, and how much might be a "real" drop in hospitalisation risk within each age group? Yes, we can, thanks to @PHE_uk‘s weekly surveillance reports, which give us an age-breakdown of admissions. gov.uk/government/sta… 5/n
[note this data has a more granular age breakdown than the dashboard, but there’s a couple of problems with it: it doesn’t reconcile back to the dashboard (there’s an unexplained c. 20% of admissions missing) and it produces some odd results for older age groups, 6/n
…including hospitalisation ratios over 100% in some weeks. But it’s the best we’ve got, so I’ve gone with it for now, and am very happy for others to improve or poke holes in the analysis. I think it’s broadly representative, but wouldn’t trust every detail. ] 7/n
This is what I get when I calculate age-specific hospitalisation ratios: as you can see, they drifted up in the early months of the year (perhaps as admission criteria became more relaxed?) and then down after Easter, as vaccination benefits kicked in strongly. 8/n

If I remove the older age groups from the graph, you can see the reductions also in the middle-aged groups’ ratios. Younger groups appear flatter, and the one group that has bucked the trend is the 0-4s who have higher ratios from May onwards (could this be a delta effect?) 9/n

But since most of the hospitalisation risk sits in the middle-aged and older groups, this is overall good news: there is a real reduction in risk happening in those groups. But there *is* still a mix effect as well; and it would be good to quantify how much is which. 10/n
The easiest way to do this is to recalculate the overall hospitalisation ratio, not with the actual age mix in each week, but with a fixed case mix (here I’ve used the most recent week). This gives us a new line on the graph (in orange), which removes the age mix effects. 11/n

Let’s ignore what happened in January because that’s probably a bit distorted by how hospitals responded to the peak of the second wave, and in particular the admission rates for older people were artificially depressed by the pressure on hospital beds. 12/n
So, looking at the blue line (the actual ratio), we can see that it fell from around 10% in early February, to around 2% now i.e. a factor of 5. Removing the age-mix effects and looking at the orange line, this fell from about 4% in February to 2% now i.e. a factor of 2. 13/n
So we might deduce that the real reduction in hospitalisation risk over the last 4 months is more like a factor of 2, not a factor of 5, and the rest is down to age-mix effects. But that’s still a significant gain. We can also examine different periods: (on the same graph) 14/n

For example, while the orange line was flat during April – meaning that the falls in the hospitalisation ratio in that period were due to age-mix effects, the orange line has fallen during May and early June – suggesting that recent falls in the ratio are more “real”. 15/n
One thing that isn’t very obvious in this data is any impact from delta, which is meant to be causing a rough doubling of hospitalisation risk. Does that mean there isn’t an impact? Not necessarily. My model (and others) suggest that, given what we know about vaccine... 16/n
…efficacy, the vaccines should have caused a real reduction in hospitalisation risk by about a factor of 4 over the last few months. Given that what we actually see is only a factor-of-2 reduction, this suggests something else is *increasing* the risk by a factor of 2. 17/n
And the obvious suspect is delta. I’m still not 100% confident in that conclusion; the timings don’t quite work how you might expect, and there’s lots of other factors that could be distorting the analysis (including case ascertainment, as @andrew_lilico has noted). 18/n
But overall I think this isn’t bad news: although falls in the hospitalisation ratio have been exaggerated by age-mix effects, there remains a significant real reduction in risk (by a factor of ~2), including the offsetting effects of delta (up) and the vaccines (down). /end
• • •
Missing some Tweet in this thread? You can try to
force a refresh














