It has been a difficult and disappointing week for many, as the rise to dominance of the delta variant has delayed plans for wider reopening; but the likely impact of delta is stark, and caution is well advised. 1/36 

We use scenario models to help NPHET and Government think quantitatively about risks and likely disease trajectories and impacts. The short form: we use a number of standard models, they are already published, and the effect of vaccination is included. 2/36
The first is a standard homogeneous population SEIR model. This considers the population, as a whole, moving between different compartments: susceptible (S), exposed (E), where you have the virus but cannot yet spread), infectious (I) and recovered (R). 3/36

The model is published here gov.ie/en/publication… and submitted for publication here arxiv.org/abs/2106.04705 4/36
The model solves the mathematical equations which govern viral transmission in a population. This largely depends on the transmissibility of the virus, the level of close social contact, and the length of time each infected person can spread the virus. 5/36

The model has been adapted to include the effect of vaccination, where we can vary assumptions on the effectiveness of vaccination in preventing asymptomatic infection, symptomatic infection, severe disease, and onward transmission 6/36

A disadvantage of these models is that they assume homogeneous mixing, so any member of the population is assumed equally likely to transmit to any other member of the population, but we know that in reality we mix within age groups, social structures and communities. 7/36
However, they have the advantage of simplicity, with fewer assumptions and parameters to calibrate, and have proved robust here and internationally in generating short- and medium-term scenario projections. 8/36
The starting point for a set of projections is to estimate the likely level of close social contact. We have a good estimate of what might happen this summer, based on our experience of last summer. 9/36
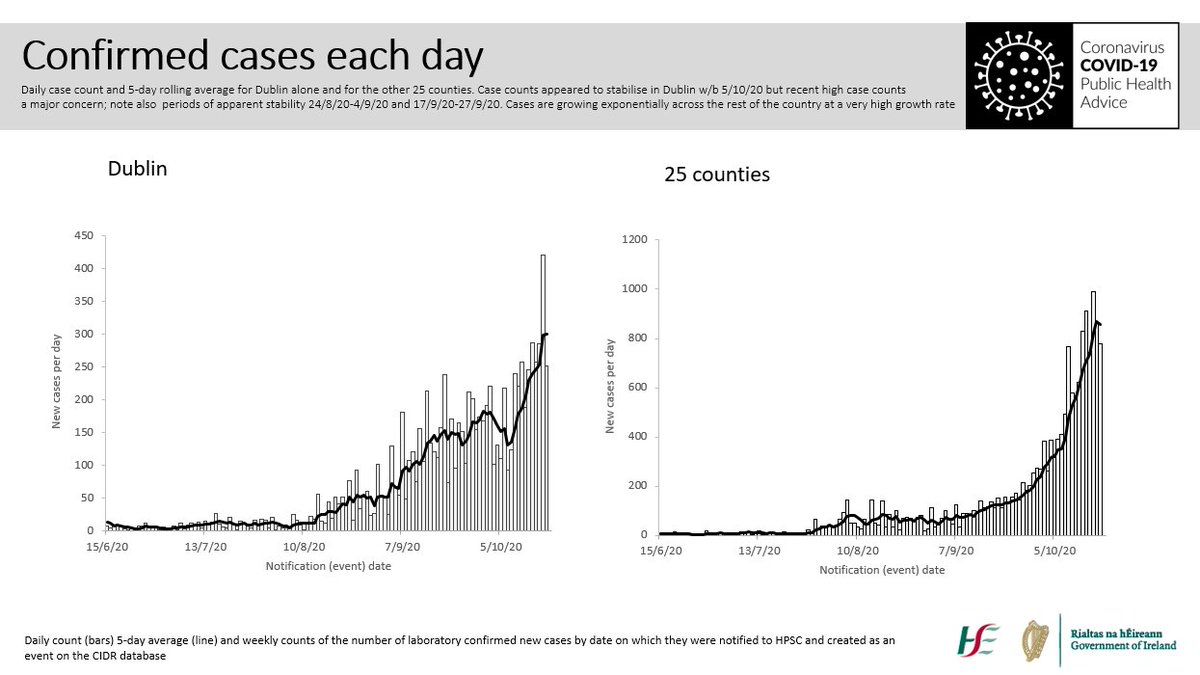
The summer 2020 reopening led to reproduction number increasing from below 1 to somewhere between 1.4 and 1.6. This began in late June 2020, and the level of viral transmission was more or less constant at this level through July and August 2020. 10/36
However, because the level of infection in late June 2020 was very low, it was weeks before the underlying exponential growth became apparent; essentially the seeds of the October 2020 surge were sown in July and August 2020. 11/36
This is our starting assumption: the level of social mixing with summer reopening could either be moderate (the level which last year gave us an R of 1.4) or high (the level which last year gave us an R of 1.6) 12/36

However, we are now dealing with a different variant, which is much more transmissible, and so the same levels of social mixing will lead to much higher levels of transmission and much faster growth in cases, which will be attenuated by progressive vaccination. 13/36
UK researchers estimate that alpha is 40-90% more transmissible than antecedents, and delta 40-60% more transmissible than alpha science.sciencemag.org/content/372/65… assets.publishing.service.gov.uk/government/upl… 14/36
ECDC estimates that delta 97% more transmissible than the strains circulating last summer, and delta 55% more transmissible that alpha, implying a lower estimate of the alpha advantage of 27% ecdc.europa.eu/en/publication…. 15/36
We therefore have two estimates of the transmission advantage of delta compared with the strains circulating last summer: conservative (1.27 x 1.55 = 1.97) and high (1.5 x 1.6 = 2.4) 16/36

We then factor in the effect of vaccination in preventing infection, using data on vaccine administration and supply as of 23 June 2021, projected forward to the end of the programme, and published estimates of vaccine effectiveness. 17/36
assets.publishing.service.gov.uk/government/upl…
assets.publishing.service.gov.uk/government/upl…
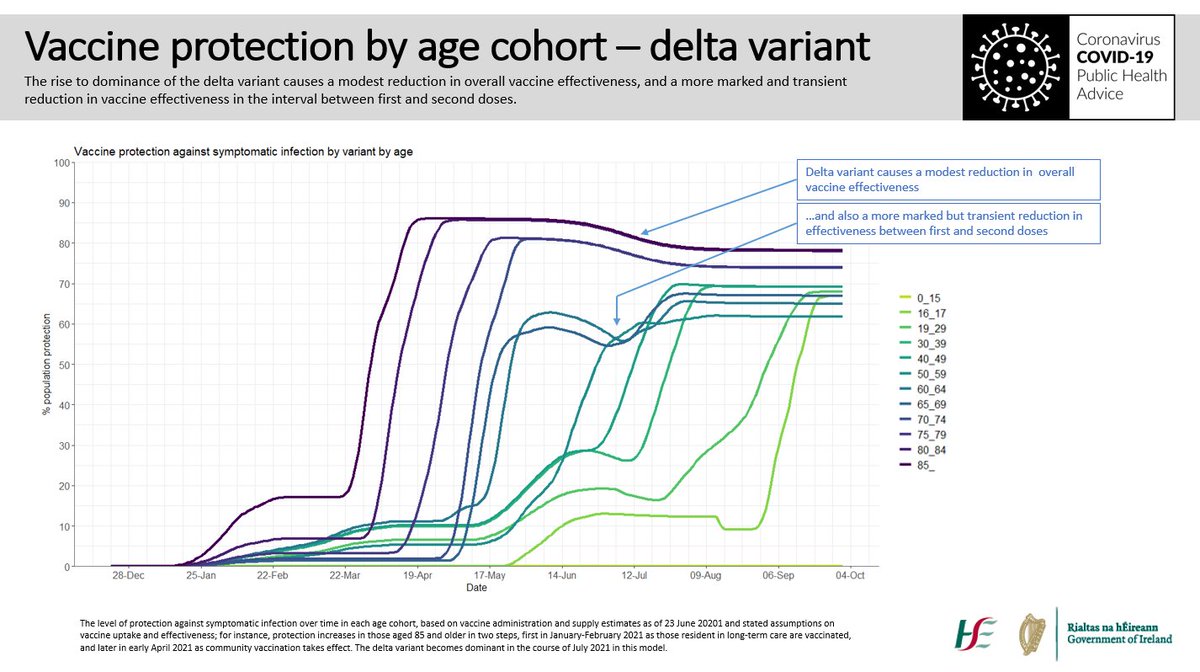
The vaccination input to the model includes the impact of delta variant on vaccine effectiveness: a modest reduction in overall vaccine effectiveness, and a more marked and transient reduction in vaccine effectiveness in the interval between first and second doses. 18/36

A counterfactual scenario, where we model with the alpha variant only, shows that without delta we could have opened on 5 July 2021 with little increase in cases or admissions. 19/36

However, even the most optimistic scenario with the delta variant shows opening on 5 July risks a significant surge in cases; note that case numbers rise very slowly through July and then surge in August and September, this being the nature of exponential growth. 20/36

It is important to note that these scenarios assume a step change in social contact from 5 July with no restrictions imposed as case numbers rise, so cases can reach very high levels; equally the increased intensity of contact and transmission into winter is not yet added. 21/36
We have two models to project hospitalisation and mortality – a simple long-term model which factors in the effect of vaccination, the age-specific risk of hospitalisation and critical care admission average length of stay and mortality rates. 22/36

We also have a more complex model which tracks short-term trends in admission probability and length of stay to support HSE planning. The latter is published here. 23/36
assets.gov.ie/89653/d2c64fd9…
assets.gov.ie/89653/d2c64fd9…
A rise in cases will inevitably lead to hospitalisation and mortality, though the rates will be far less than we experienced without vaccination; nonetheless a long wave of disease leads to a significant number of adverse outcomes. 24/36


While 70-80% of cases will be in people under 40, there will be a lot of infections and a lot of adverse outcomes in people over 40; about 70% of the hospitalisations and over 99% of the deaths would be in people over 40. 25/36
Why would this happen if everyone is vaccinated? Vaccines offer extraordinary protection, but not perfect. We have almost 500,000 people aged 70 and over; even if the vaccine is 95% effective in preventing severe disease, 25,000 people remain vulnerable. 26/36
The first central scenario shows a worrying possibility. The assumptions here are not unreasonable – slightly higher levels of social mixing and conservative estimates of transmission advantage. 27/36



The second central scenario is moderate levels of social mixing (the lower end of what we had last summer) but a higher transmission advantage for delta 28/36

We compared the outputs of homogeneous population SEIR with an age-cohorted SEIR model, where higher levels of mixing occur within age groups than between age groups. One of the calibration methods used for this model is published here: doi.org/10.1016/j.epid… . 29/36

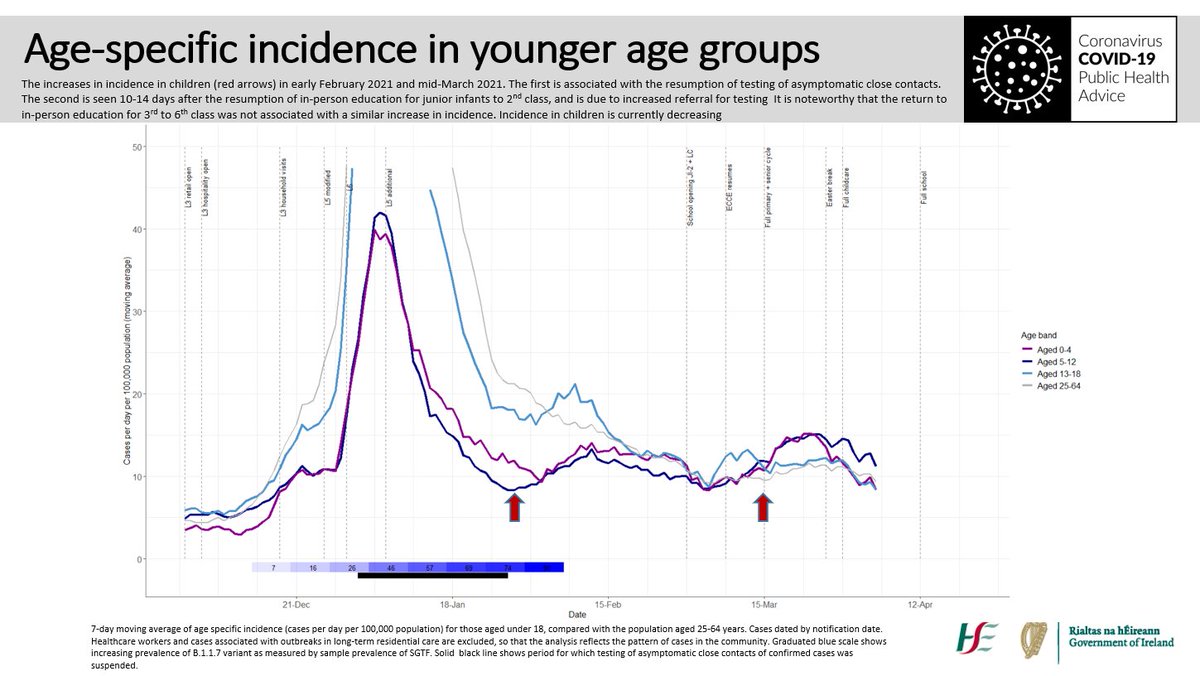
These models show that cases are concentrated in younger age groups; they give lower estimates overall because the model structure and calibration are different, and because social mixing is concentrated within age groups. 30/36

If children and adolescents are less susceptible to infection, or less likely to infect others, the wave of infection will develop more slowly and the peak will be lower; the role of children in transmitting the infection will become clearer as more adults are vaccinated. 31/36
Finally, we use an agent-based model, where social structures and transmission are simulated in detail at the individual level; these show rapid spread in younger people with transmission into older groups, and highlight uncertainty on the role of children and adolescents. 32/36
The agent-based models also illustrate the random component in epidemic trajectories, that a small number of super-spreader events can alter the overall incidence. 33/36
The full set of scenarios include a pessimistic scenario; while less likely than the central scenarios, the assumptions are a level of social mixing as occurred at the end of last summer, and transmission advantages for alpha and delta as reported from the UK. 34/36

All this illustrates one thing: a variant with a transmission advantage can do very significant damage if we let it spread in a partially vaccinated population, the scale of the damage depends on the transmission advantage, and it starts slowly and escalates rapidly. 35/36
My sincerest thanks to the many colleagues who have done extraordinary work of international quality over the last 15 months, but with particular intensity over recent weeks, to provide valuable tools to support a critical and very difficult decision. 36/36
• • •
Missing some Tweet in this thread? You can try to
force a refresh