1/ We studied the quality,
quantity and persistence of #SARSCoV2 antibodies in primary school students (6-11 year-olds) compared to staff (adults) over 6 months (until ~7-8 months after their #SARSCoV2 infection)
Here’s what we found (pre-print) 🧵
👉 medrxiv.org/content/10.110…
quantity and persistence of #SARSCoV2 antibodies in primary school students (6-11 year-olds) compared to staff (adults) over 6 months (until ~7-8 months after their #SARSCoV2 infection)
Here’s what we found (pre-print) 🧵
👉 medrxiv.org/content/10.110…
2/ The proportion of students & staff who had #SARSCoV2 antibodies in back June 2020 was similar:
👉 11.5% (95%CI, 9.4-13.9) & 11.3% (95%CI, 9.2-13.6; p=0.88) students had nucleoprotein & RBD antibodies vs 15.6% (95%CI, 13.7-17.6) & 15.3% (95%CI, 13.4-17.3; p=0.83) staff
👉 11.5% (95%CI, 9.4-13.9) & 11.3% (95%CI, 9.2-13.6; p=0.88) students had nucleoprotein & RBD antibodies vs 15.6% (95%CI, 13.7-17.6) & 15.3% (95%CI, 13.4-17.3; p=0.83) staff
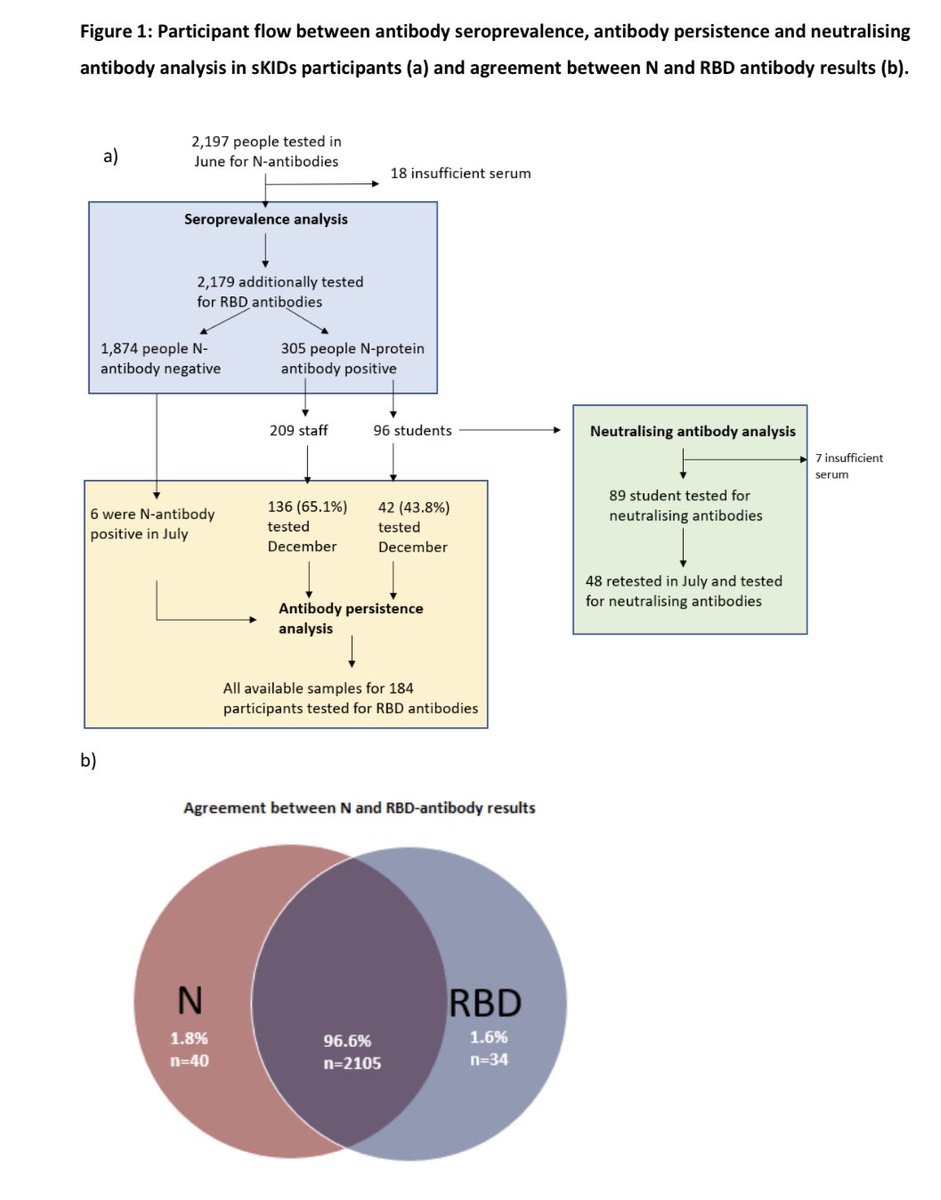
3/ Live virus neutralising activity (ability of antibody to kill #SARSCoV2) was detected in 79.8% (71/89) of N antibody & 85.5% (71/83) of RBD antibody positive kids. RBD correlated more strongly with neutralising activity (rs=0.75; p<0.0001) than N antibodies (rs=0.37; p<0.0001)
4/ After 6 months, 58% (107/184) of participants lost their N antibody vs 21% (33/158) for RBD antibody (p<0.001). There’s something about Abbott N assay that loses positivity over time. Others N assays remain positive with time. That’s why we retested all samples using RBD assay

5/ Importantly though, the proportion of students & staff who lost their #SARSCoV2 antibodies more than 6 months after their infection was small similar between students and staff for both N (p=0.26) and RBD-antibodies (p=0.43) 👉 medrxiv.org/content/10.110…

6/ Interestingly, the amount (titres) of N (p=0.028) & RBD (p<0.0001) antibodies back in June 2020 were significantly higher in students than in staff but ended up at similar levels after 6 months in December 2020 (p=0.16 & p=0.37, respectively)
👉 medrxiv.org/content/10.110…
👉 medrxiv.org/content/10.110…

7/ In conclusion, young children are able to mount strong immune responses against #SARSCoV2 (better than adults) even if most of them have asymptomatic infection. They are also able to retain their immunity for >6 months, at least as well as adults
👉thelancet.com/journals/lanch…
👉thelancet.com/journals/lanch…
• • •
Missing some Tweet in this thread? You can try to
force a refresh