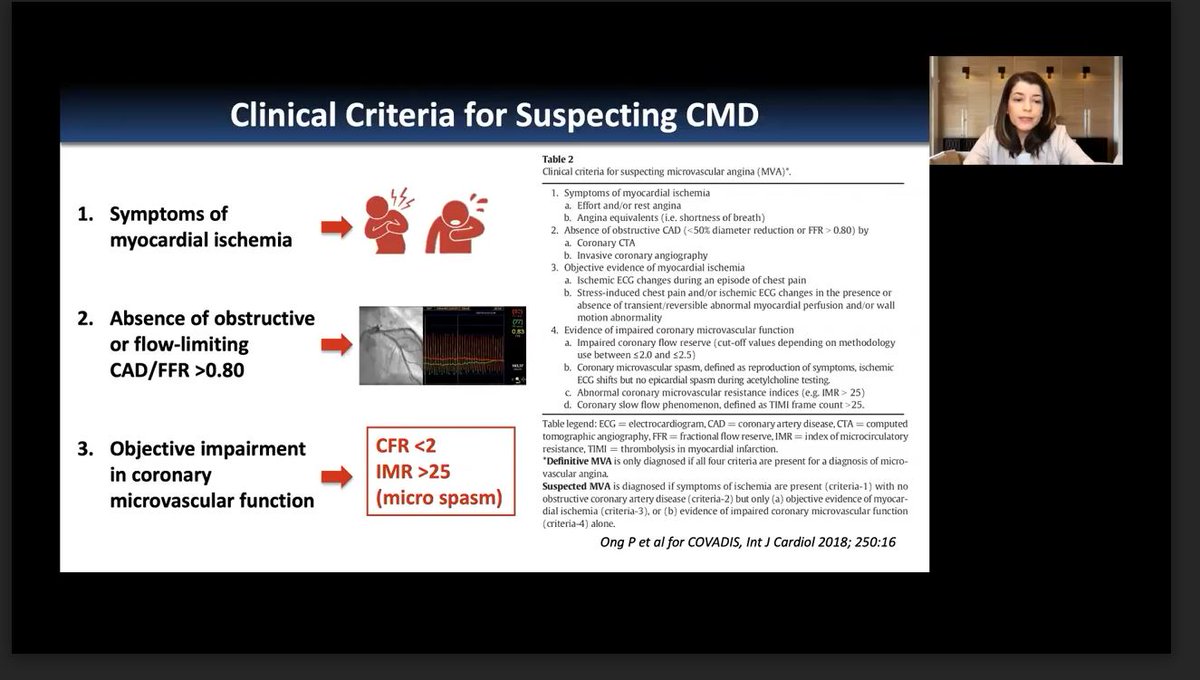
Obstructive CAD is just one etiology of ischemia. If no obstructive disease, consider coronary microvascular dysfunction #CMD. So what is best imaging modality for CMD? @VTaqMD #SCCT2021 




How to evaluate for #CMD? A multidimensional cardiac stress PET test can evaluation for perfusion, function, and coronary blood flow. @VTaqMD #SCCT2021


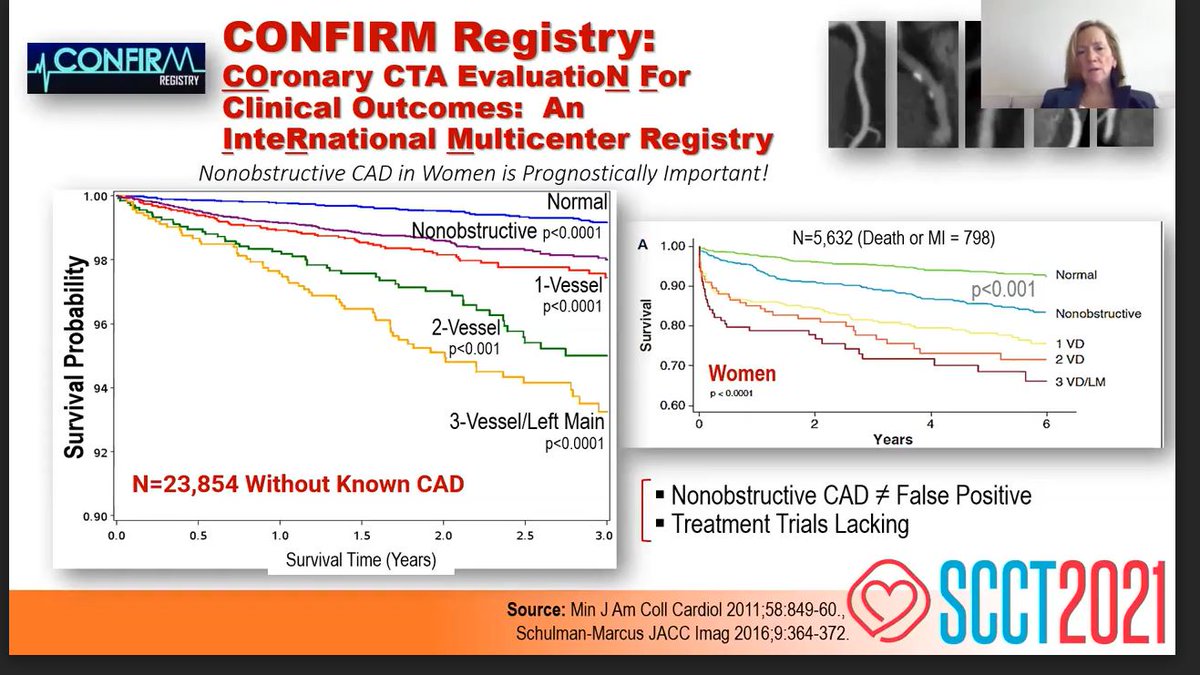
Distribution of risk by coronary flow reserve #CFR. Even in absence of inducible ischemia or obstructive lesions, impaired CFR is associated with increased CVD risk. When severely impaired, CFR more prognostically significant in women. @VTaqMD #SCCT2021




#CMD is prevalent. #CFR <2 is prognostic of risk. Patients with low CFR plus elevated troponin, or low CFR with elevated E/e’, had even worse prognosis. @VTaqMD #SCCT2021




CMD is associated with worse prognosis in obesity than BMI alone. PET and CCT offer complementary information about risk. CMD also interactions with macrovascular disease. @VTaqMD #SCCT2021



Would a diagnosis of #CAD, not just #CMD, influence management? In setting of known CAD, would a diagnosis of CMD influence management? And top 3 takeaway points about CMD by @VTaqMD #SCCT2021



• • •
Missing some Tweet in this thread? You can try to
force a refresh