#YesCCT : Clinical reporting & understanding finance by @docjuanb at #SCCT2021 . There are reimbursement challenges . #Cardiac CT is in the wrong Ambulatory Payment Classification (APC). Bill also must be supported by clinical symptom & diagnostic ICD10 codes. Not a “rule out”. 




Reimbursement tracks with the CPT used so use the right CPT code and make sure language in report supports that code. All CTA assumes 3D, thus need to mention 3D in report. Have your reporting align with @Heart_SCCT guidelines. @docjuanb at #SCCT2021



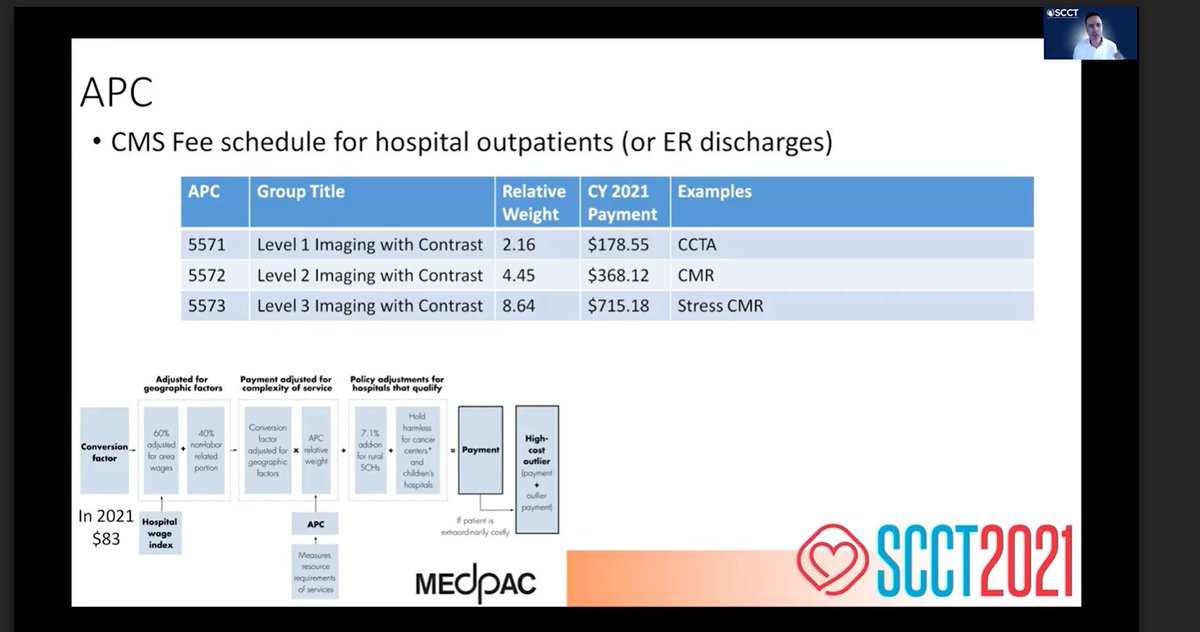
Unfortunately #cardiacCT often lumped into CT not cardiac. Hospitals should update cost charges to accurately reflect true cost of work, align w/ other cardiac testing. With costs underreported, CMS bases APC & reimbursement on these historically lower costs @docjuanb #SCCT2021



• • •
Missing some Tweet in this thread? You can try to
force a refresh