Now up, growing your program through modern media by @purviparwani. In current era, #SoMe is a powerful tool for growing your program. #SCCT2021 




Strategies for growing your growing your advanced imaging program through modern media. Great talk by @purviparwani #SCCT2021




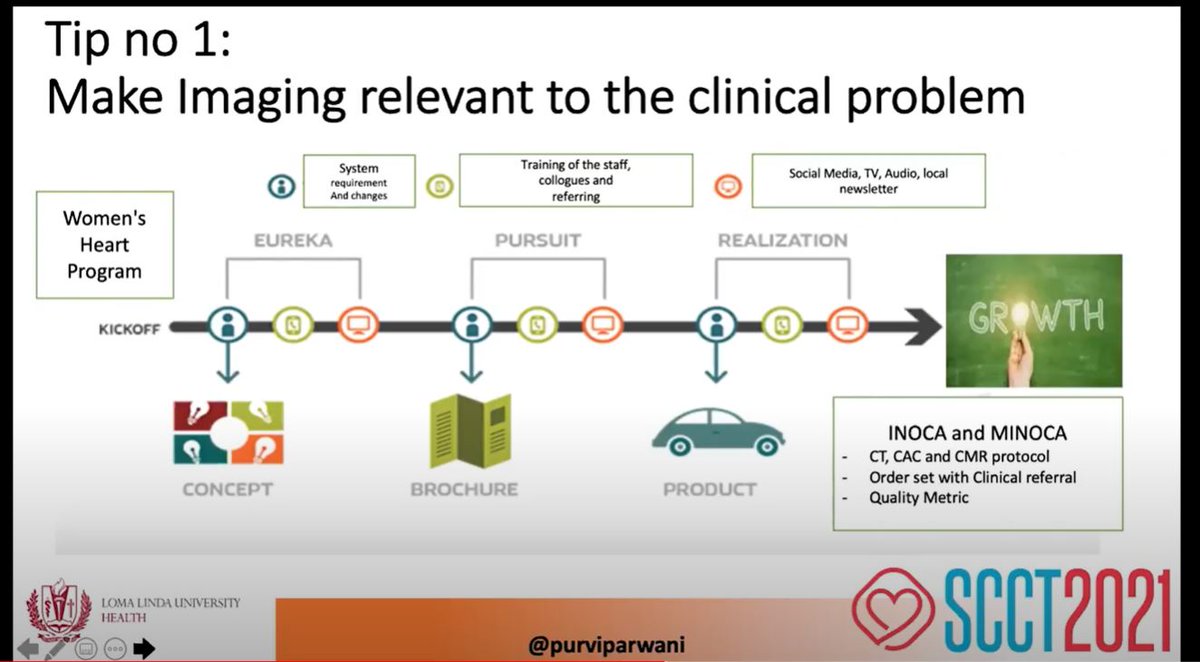
5 tips for growing #CardiacCT program @purviparwani #SCCT2021. Tip 1: Make imaging relevant to clinical problem. Tip 2: Imaging content on #SoMe. Tip 3: 80/20 rule of original content/promotion. Tip 4: 360 degree Marketing



5 tips for growing #CardiacCT program @purviparwani #SCCT2021 Tip 5: content is key. Disseminate. Finally track impact through Altmetrics. And...the summary slide



• • •
Missing some Tweet in this thread? You can try to
force a refresh