
1/n
🧵 about RSV, COVID, and grifting
Social media grift in the name of “public health” begins anew on the eve of school openings.
The expected July-Aug Sun Belt surge coincided with “Delta” => good times for politicized fear porn.
But there’s more to the story…
🧵 about RSV, COVID, and grifting
Social media grift in the name of “public health” begins anew on the eve of school openings.
The expected July-Aug Sun Belt surge coincided with “Delta” => good times for politicized fear porn.
But there’s more to the story…
https://twitter.com/cleavon_md/status/1422322641097142275
2/n
Delta has been the dominant strain in many states since June.
The quoted doctor claims no pre-existing condition in half (debateable) implying something new afoot.
Yet the UK did not see a spike in Pediatric disease, or general virulence, with its now waning Delta wave:
Delta has been the dominant strain in many states since June.
The quoted doctor claims no pre-existing condition in half (debateable) implying something new afoot.
Yet the UK did not see a spike in Pediatric disease, or general virulence, with its now waning Delta wave:

3/n
So what is new?
There’s a spike in viruses that present a much bigger risk to kids. RSV positivity in the Sun Belt is >30% and we are having an unseasonal surge in several viruses … globally. Compare Aug ‘20 to Aug ‘21.
These viruses routinely affect healthy kids.
So what is new?
There’s a spike in viruses that present a much bigger risk to kids. RSV positivity in the Sun Belt is >30% and we are having an unseasonal surge in several viruses … globally. Compare Aug ‘20 to Aug ‘21.
These viruses routinely affect healthy kids.

4/n
RSV is unseasonally surging nationally — and globally.
It’s the most common severe respiratory infection in infants and causes 66k deaths worldwide annually.
RSV is unseasonally surging nationally — and globally.
It’s the most common severe respiratory infection in infants and causes 66k deaths worldwide annually.



5/n
RSV is particularly up in many of the Sun Belt states that are always mentioned by the media and politicized “experts” like @PeterHotez and blue check social media doctors like @Cleavon_MD whose post inspired this thread.
RSV is particularly up in many of the Sun Belt states that are always mentioned by the media and politicized “experts” like @PeterHotez and blue check social media doctors like @Cleavon_MD whose post inspired this thread.




6/n
And there are spikes in metapneumovirus almost everywhere except the Northeast.
And there are spikes in metapneumovirus almost everywhere except the Northeast.


7/n
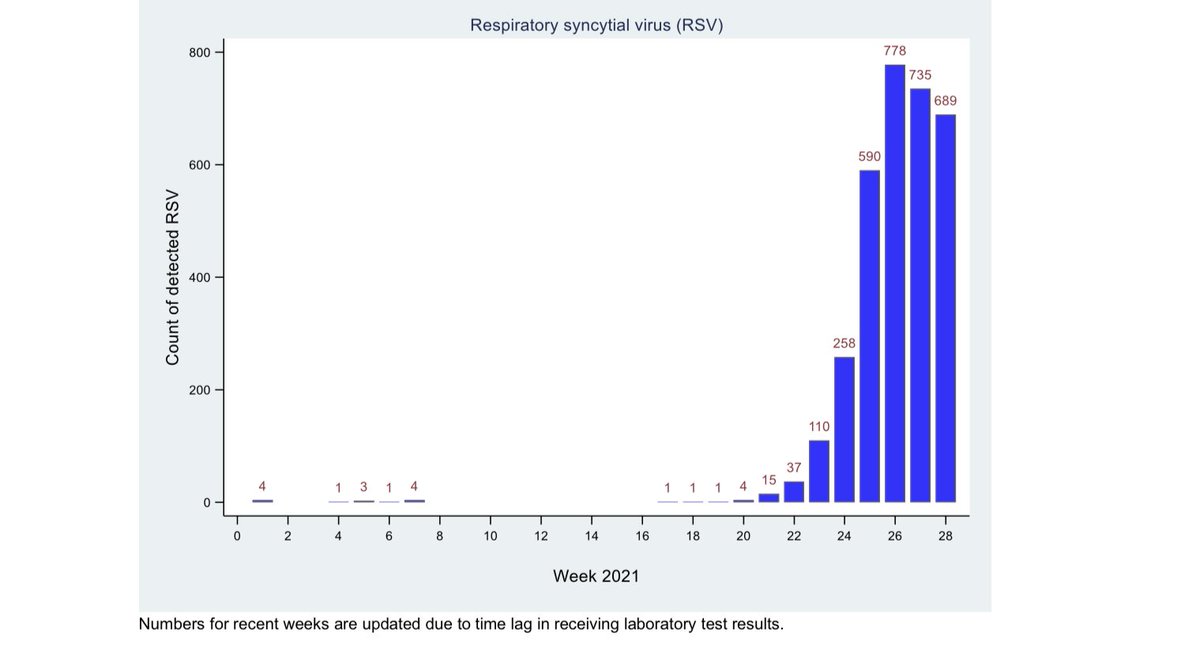
The UK is experiencing and ongoing and accelerating unseasonal spike in RSV and other viruses as their Delta wave wanes. New Zealand’s unusual RSV spike appears to have peaked.
The UK is experiencing and ongoing and accelerating unseasonal spike in RSV and other viruses as their Delta wave wanes. New Zealand’s unusual RSV spike appears to have peaked.

8/n
So why is all of this important?
Because coinfection with RSV and SCoV2 will make it seem like there’s a spike in C19 Pediatric disease, when it may not be the culprit. There’s nothing about RSV that makes it clinically distinct from C19 — except higher severity in kids.
So why is all of this important?
Because coinfection with RSV and SCoV2 will make it seem like there’s a spike in C19 Pediatric disease, when it may not be the culprit. There’s nothing about RSV that makes it clinically distinct from C19 — except higher severity in kids.
9/n
So why is there an unseasonal spike in RSV?
Theories abound including “weakening” of the immune system w/ 18m of isolation.
We all are exposed to RSV in childhood. By 2yo, 80% of kids have had at least 1 RSV infection (2/3 in the 1st year of life). Reinfection is common.
So why is there an unseasonal spike in RSV?
Theories abound including “weakening” of the immune system w/ 18m of isolation.
We all are exposed to RSV in childhood. By 2yo, 80% of kids have had at least 1 RSV infection (2/3 in the 1st year of life). Reinfection is common.
10/n
There is also some interesting research around RSV “latency”: it “hides out” in our cells.
erj.ersjournals.com/content/46/sup…
There is also some interesting research around RSV “latency”: it “hides out” in our cells.
erj.ersjournals.com/content/46/sup…
11/n
The main point of this 🧵 is to arm you with context and data as the grifters scream louder.
If their purpose is to promote vaccination, then it should be done without fear.
That they pump fear without context on the eve of much needed school openings is immoral.
The main point of this 🧵 is to arm you with context and data as the grifters scream louder.
If their purpose is to promote vaccination, then it should be done without fear.
That they pump fear without context on the eve of much needed school openings is immoral.
12/n
@Cleavon_MD has been a doctor for fewer months than my number of years in the ER.
He’s mostly about his media profile and politicizing the pandemic.
Play along if you want to sacrifice the well being of children for another year.
Alternatively, reject this cynical game.
@Cleavon_MD has been a doctor for fewer months than my number of years in the ER.
He’s mostly about his media profile and politicizing the pandemic.
Play along if you want to sacrifice the well being of children for another year.
Alternatively, reject this cynical game.
13/n
Some mentions who can provide further context to this thread:
@ID_ethics
@MartinKulldorff
@covidtweets
@kerpen
@justin_hart
@Emily_Burns_V
@sdbaral
Some mentions who can provide further context to this thread:
@ID_ethics
@MartinKulldorff
@covidtweets
@kerpen
@justin_hart
@Emily_Burns_V
@sdbaral
14/n
References:
assets.publishing.service.gov.uk/government/upl…
cdc.gov/surveillance/n…
esr.cri.nz/assets/SHIVERS…
cdc.gov/surveillance/n…
assets.publishing.service.gov.uk/government/upl…
ncbi.nlm.nih.gov/pmc/articles/P…
References:
assets.publishing.service.gov.uk/government/upl…
cdc.gov/surveillance/n…
esr.cri.nz/assets/SHIVERS…
cdc.gov/surveillance/n…
assets.publishing.service.gov.uk/government/upl…
ncbi.nlm.nih.gov/pmc/articles/P…

• • •
Missing some Tweet in this thread? You can try to
force a refresh










