While I'm grateful that JCVI are advising vaccinating all 16-17 yrs, this delay has been costly. We're still behind vaccine policy in other countries for 12-15 yr olds. Our preprint out today shows benefits far outweigh risks for 12-17 yr olds in England🧵
osf.io/grzma
osf.io/grzma
Our preprint with @chrischirp @martinmckee @trishgreenhalgh @tomlincr @ReicherStephen @SusanMichie @Sethflaxman @Kit_Yates_Maths @globalhlthtwit @GabrielScally @HZiauddeen @SpirosDenaxas @SGriffin_Lab @DrZoeHyde Samir Bhatt, Oliver Ratmann -a quantitative risk vs benefit analysis
The UK strategy is out of line with many other countries, including US, Israel, and much of Europe & SE Asia that have prioritised vaccination of all 12-17 yr olds. >9 million adolescents have been vaccinated in the US alone, and benefit vs risks have been quantified carefully.
The CDC took pains to quantify benefit vs risk based on exposure levels in the US at the time, and provided clear numbers on hospitalisations, and vaccine associated myocarditis so risk could be directly assessed.
Even without considering long COVID numbers, they concluded benefit was far higher than risk. The additional benefits in terms of reducing community transmission, educational disruption & variant evolution make the argument even stronger.
cdc.gov/vaccines/acip/…
cdc.gov/vaccines/acip/…
We did a similar analysis for England using hospitalisation, ICU admission and death rates from 1st July 2020- 31st March 2021 in England. Based on current incidence rate from the PHE, we estimated what the benefits & risks of vaccinating all 12-17 yr olds would be over 16 weeks.
We also consider the risk of rare vaccine associated myocarditis(30-40/million with Pfizer 2nd doses). We know that this is usually mild with most cases resolving with minor treatment (compared to COVID-19 hospitalisations which can leave children with long-term neuro disease)
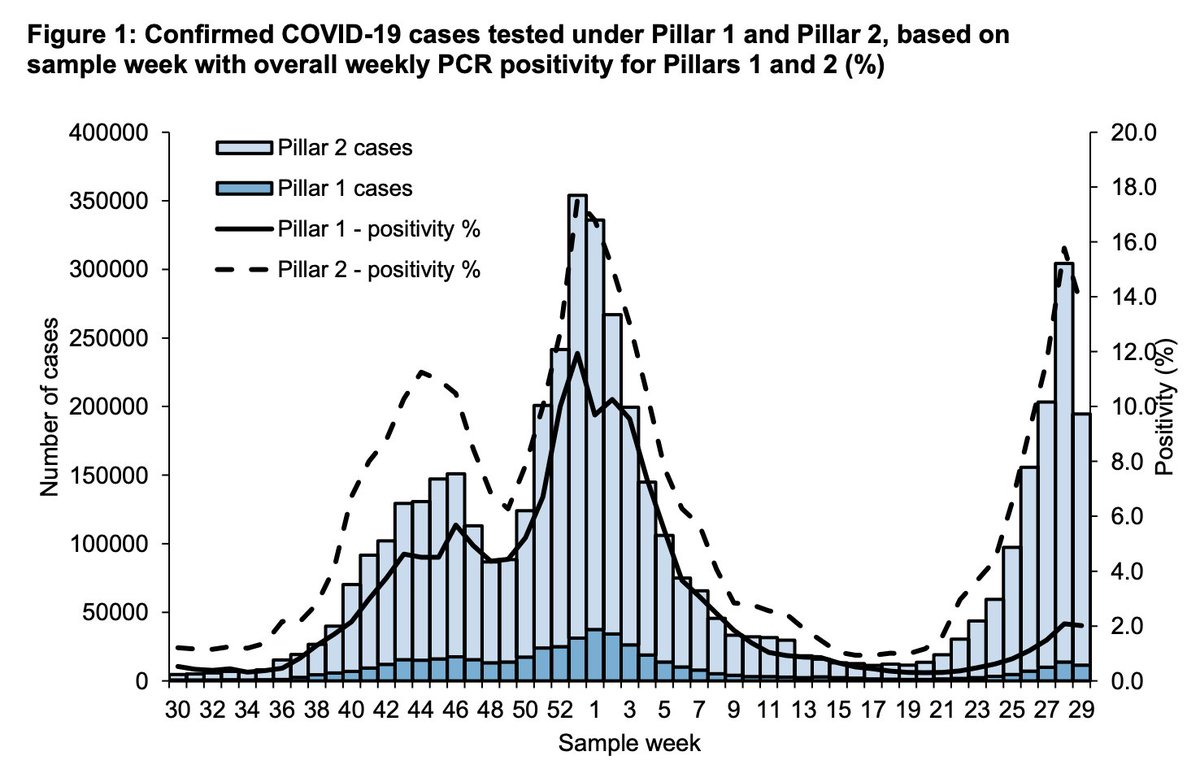
Essentially, we calculated what might happen if all 3.9 million 12-17 yr olds were vaccinated before Sept, and rates continued at 1000/100,000/wk (wk 29 data) throughout 16 weeks till end of term in December. We also looked at a 20x lower incidence to see if this changed results.
Our results show that at current high incidence rates, vaccination of all 12-17 yr olds prevents thousands of hospitalisations, cases of long COVID (considering either 4% or 8% incidence) and deaths, and benefits *far outweigh* risks from vaccine associated myocarditis. 

We find even if we look at a 10-20x lower rate than currently i.e. 50/100000/wk, which is comparable to the much lower rate recorded end of April 2021, the benefits to 12-15 yr olds still greatly outweigh the risks.

In these analysis we made the worst-case assumption that all cases of vaccine-associated myocarditis are hospitalised, and we still find that on hospitalisations benefits always outweigh risks unless we have very low incidence rates at a level that have not been seen in 2021.

Our assessment of vaccine effectiveness is conservative (64% in preventing long COVID - no additional protection apart from preventing infection, and 90% for severe disease), and we haven't considered the data for hospitalisations post-delta, which may lead to more severe disease
Even when we consider lower incidence (4%) of long COVID as reported today- despite the many flaws of this report- we still find at current rates 16000 cases of long COVID would be averted over a 16 wk period if we vaccinated all 12-17 yr olds.
We also consider lower case hospitalisation rates (0.5%) than the ones estimated from within our data, and still find benefits outweigh risk with respect to hospitalisations unless we get to rates of 50-60/100K/wk or below (current rates at least 10x higher)
And let's remember, none of this even considers the many additional benefits of vaccinating children, including protecting the wider community by reducing transmission, protecting the immunosuppressed, reducing educational disruption & the potential for variant evolution.
I think it's vital that the JCVI articulate very clearly and transparently what their risk-benefit analysis is on vaccines. Their public statement does not provide any quantitative analysis of this unlike the very clear analysis by the CDC, and now our analysis as well.
It's important that risk-benefit analysis is based on clear evidence and numbers rather than vague statements about risks and benefits that are not quantified. This is also v. important to engender public trust, which is important for vaccine uptake.
I hope the JCVI will, based on this, also extend vaccines to all 12-15 yr olds. It's unfortunately too late to vaccinate all before school openings, but we must protect children through vaccination & mitigations in schools as far as possible, before reopening in Sept.
The JCVI need to articulate very clear evidence for why they aren't planning to do this, if they aren't, because it seems that the benefits are likely substantially greater than the risks.
While our analysis is England focused (because we used England data), it can be easily adapted to other nations. We provide our analysis here, so anyone can use it, and adapt accordingly:
github.com/dgurdasani1/va…
github.com/dgurdasani1/va…
• • •
Missing some Tweet in this thread? You can try to
force a refresh