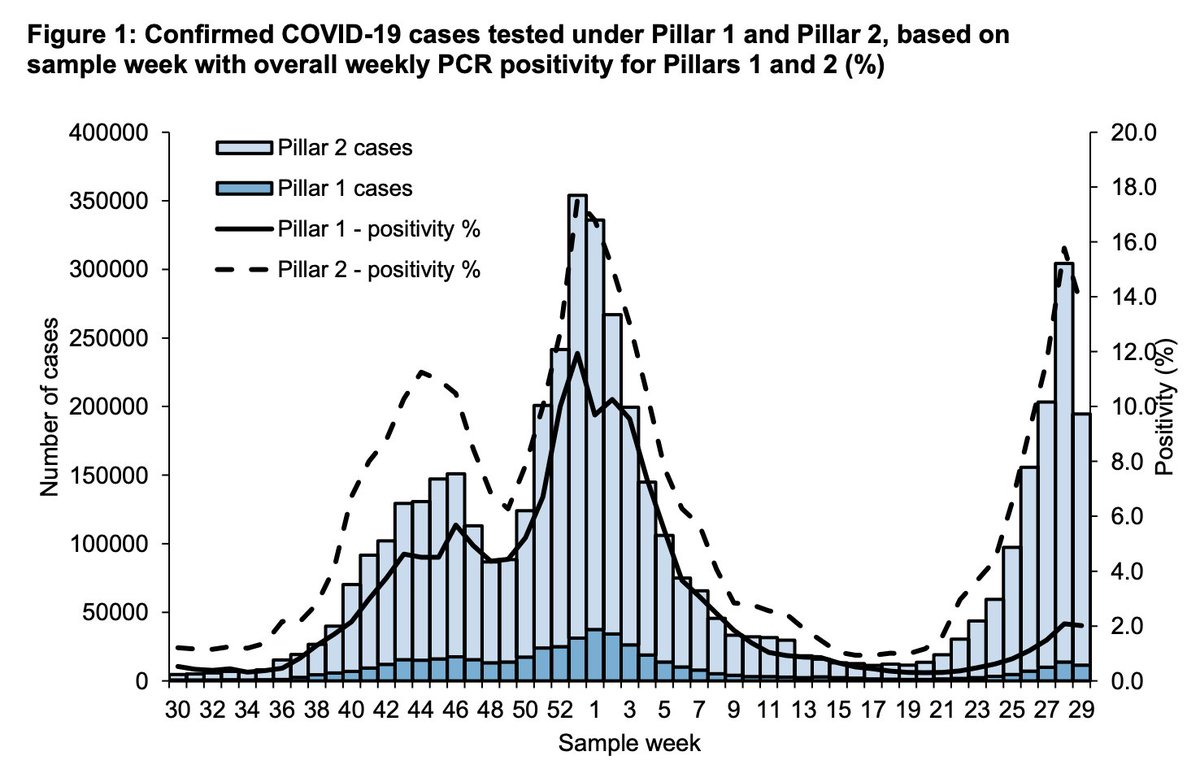
The PHE report released yesterday shows inconsistencies between case rates in England & positivity (the proportion of tests that are positive). This together with ONS data today suggests that at least some of the steep drops in cases we're seeing are down to less testing.🧵
First, let's compare case incidence to positivity rates. Case incidence depends on overall number of positive COVID-19 cases found each week. Positivity looks at proportion of tests that were positive. Case numbers will depend on background incidence & level of testing.
Positivity can help us when tests are declining, because cases found can come down when people aren't being tested for whatever reason. But positivity should remain high. The PHE report shows sharp declines in cases, but only very recent plateauing/slight decline of positivity. 
It does appear that we have seen declines in numbers of PCR and LFD tests being done in the past two weeks- sharper in the past week.
So, what age groups are showing this discrepancy between declining cases & positivity levels the most? Comparing the left plot (case rates) with positivity shows stark differences in school age groups esp 10-19 yr olds. While cases show huge declines, positivity shows steep rises


So, the trends actually look very different when we look at case rates, vs proportion of tests that are positive (positivity). This suggests that case rates are unreliable, esp for these groups & are perhaps showing decline due to low testing while positivity is actually rising.
How do we make sense of this?
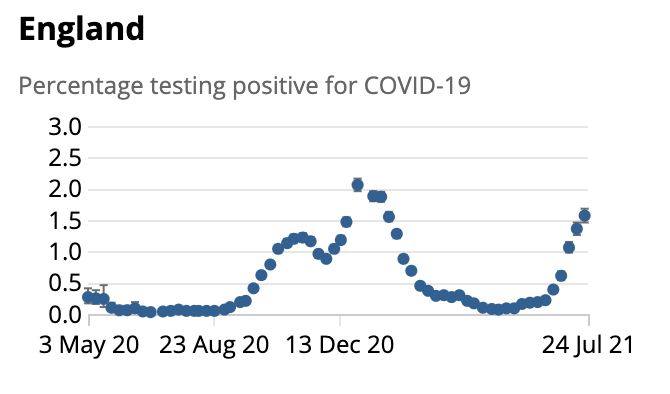
To understand real trends that aren't dependent on testing behaviour, we ideally need to look at random community surveys that don't depend on people coming forward for testing. Let's look at the ONS survey out today that does just this.
To understand real trends that aren't dependent on testing behaviour, we ideally need to look at random community surveys that don't depend on people coming forward for testing. Let's look at the ONS survey out today that does just this.
Despite v. sharp declines in reported cases from the 16th July, ONS data published up to the 24th still shows a rise in prevalence of infection. In fact when we look at prevalence by age, we see the same patterns we saw on positivity- - rises in both primary & 2ndary school gps

It also shows early decline/plateauing in other age groups (in line with the declines in positivity seen), but not the sharp declines that are suggested by age-specific case numbers. This suggests possible declines/plateauing in non-school age groups by the 24th July.
The impact of school closures on school age groups is expected to be seen in next weeks ONS data which will include surveys up to the 30th July (given schools closed on the 22nd July).
Let's look at data we have from other sources now.
Let's look at data we have from other sources now.
The Zoe symptom tracker also suggests cases have been rising until v. recently & it has been recording much higher cases than those reported (in the 60,000 range rather than the reported 30,000 range). Recent data suggests plateauing or early declines - consistent with positivity


So what's going on with testing?
I don't know - the recent CORSAIR study in it's June surveys showed that of those who were symptomatic in England & Wales, only 1 in 3 got tested- 53% with PCR and 44% LFT. This was even before we started seeing the July declines in testing.
I don't know - the recent CORSAIR study in it's June surveys showed that of those who were symptomatic in England & Wales, only 1 in 3 got tested- 53% with PCR and 44% LFT. This was even before we started seeing the July declines in testing.
I'm not sure if testing behaviour has changed more recently - or what may have led to lower levels of testing, and the sort of underestimation of case rates we're seeing now.
Another question worth addressing here is why we aren't seeing rises from opening up on the 19th July
Another question worth addressing here is why we aren't seeing rises from opening up on the 19th July
Changes following removal of mandatory restrictions will depend a lot on how much behaviour changes, and how quickly. This is likely to be a gradual rather than sudden change (although events like nightclubs opening and large gatherings are likely to have more immediate effects)
Mobility data has shown gradual increases in activity - with no clear increase apparent since 19th July, and is still below pre-lockdown levels. This is not unexpected, & mobility data doesn't give a full picture but just highlights that changes in behaviour are often gradual.

Part of the decline in cases over the past few weeks seems to potentially be related to the surge following Euro2020 ending. This is reflected in the stark differences in positivity, and recent declines in young men and women (yellow line in plot below).

Of course school closures last week will likely help bring cases down as well given schools have been contributing considerably to transmission, especially with the delta variant, with positivity being highest in 2ndary school children & young adults.
What happens in the coming weeks will depend a lot on how much school closures offset the changes in behaviour following 19th July - which will depend a lot on the extent, and rapidity of change in behaviour. The govt strategy has led to a lot of uncertainty about the future.
The discrepancies between cases reported, positivity, symptom tracking (Zoe), and prevalence estimated through the ONS is worrying - this suggests that a lot of people aren't getting tested recently & that cases are not a reliable indicator currently.
I'm not sure why that is, but it's important that the government convey the importance of testing in its messaging. The fact that it seems to be dropping isolation for contacts <18yrs, and the vaccinated, & some frontline workers may send the message that the pandemic is over
The fact the govt has moved to remove most mandatory restrictions, and the media discussion of the 'pingdemic' rather than the 'pandemic', treating isolation as a nuisance rather than a necessity may also have sent the message that testing isn't important.
Lack of support with isolation has already meant that most symptomatic people don't get tested, but this may get even worse over time, which means we will not be breaking most chains of transmission, because we just won't be identifying them.
It's also very clear that our eligibility criteria for testing are very outdated. We aren't testing for 2 of the 3 most common symptoms of COVID-19 currently, which will lead to further underestimation of cases:
https://twitter.com/fascinatorfun/status/1420406810717179904?s=20
I think the picture will get clearer over the coming week, as cases should be followed by a decline in hospitalisations, and the timing, and extent of this will tell us retrospectively about case declines. In scotland there was a 14-15 day lag between cases & admissions declining
This means we should start seeing declines in admissions next week - it'll be key to see when these start & how steeply they decline. Long term trends aren't clear, but it's clear that we need to rely on more than case numbers, because the picture is more complex than it appears.
What is clear is that Euro2020 and schools have both been contributing considerably to transmission. This is also clear from data from Scotland where cases declined after schools closed and Scotland dropped out of the Euro2020s. Same gender gaps in cases were seen there too.
This should at the v. least send a signal to govt about the recklessness of allowing large gatherings & not putting in place safety measures in schools or vaccinating adolescents ahead of September.
We have amazing surveillance systems in the UK- but they mean nothing if we don't act on them.
Just want to add that as outlined here ONS prevalence is a lagging indicator, so interesting that we're seeing age-based trends line up between ONS & positivity- but it'll be important to follow ONS over the coming wks to get an idea of extent of decline.
https://twitter.com/jburnmurdoch/status/1421117165319725056?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh