
Seeing a lot of minimisation of long COVID again by the usual players based on recent ONS data - interesting that the same people suggesting no one understand ONS methodology, don't seem to have questioned why ONS estimates have changed as much as they have, or what they mean.🧵
So let's get right to it. The ONS infection survey is a very good survey for infection and picks this up through sampling random households in the community. The long COVID survey looks at those who tested positive ~21K people, and compares them to matched controls who were -ve
They ask both groups to answer question about whether they have 1 in 12 symptoms. These symptoms are limited, and don't include things like brain fog, or mood changes, or palpitations, and many other common symptoms of long COVID.
Patient groups have been working with the ONS to help expand their symptoms list, and I believe they are planning to do this in the future.
Why is this important?
Why is this important?
Previous studies (e.g. the Zoe study) which also very likely underestimated long COVID, for several reasons, have found that when symptoms like brain fog, and mood symptoms are actually included in the survey, they are very common (occur in 11% & 15% of older kids).
Clearly if you don't include these, you'd vastly underestimate the prevalence of an illness, because you just weren't asking about the common symptoms within that syndrome. In fact, it's very clear that prevalence estimates in studies depend on capturing these symptoms.
For example, compare ONS adult estimates with those in the REACT-1 study, which did a similar analysis, on a much larger sample, assessing 29 symptoms, and is also based on a random community survey, and found 37% of *symptomatic* cases had persistent symptoms for 12 weeks.
The Clock study - which is the largest study on this so far, looking at a much larger set of >40 symptoms found 1 in 7 children had persisting symptoms for 15 weeks or more. There were limitations to the study, given the low participation, and biases could go either way.
It depends on whether healthy people are more likely to participate and follow up on surveys (this is often the case), or whether people who are ill are more likely to participate (not often the case, but still possible in this context)
Studies that do not explicitly ask for specific symptoms or ask for a limited set always show lower estimates of long COVID- the Virus Watch study from GOSH did not ask any specific questions- just an open ended one- and the estimate of long COVID there was ~4% in children
There is clearly an association between how comprehensive the list of symptoms is and how much long-term illness is captured. And let's be very clear - this isn't down to *background* symptoms.
The Clock study had a control group and despite a significant proportion of them having these symptoms, the symptoms in those post-COVID-19 were two times those in controls. Even the ONS with it's limited definitions had a several fold difference between cases & controls. 

Some will suggest that this is due to 'recall bias' - that those people who have had COVID-19 will just recall and report symptoms more. While that is a possibility, it certainly doesn't explain why the ONS found that viral loads were higher among those likely to have long COVID

An association of lower Ct values (higher viral loads) with symptom persistence seems to suggest either a biological relationship between viral loads and persistence, or potentially that PCRs were done earlier in this group, because they were more likely to be symptomatic.
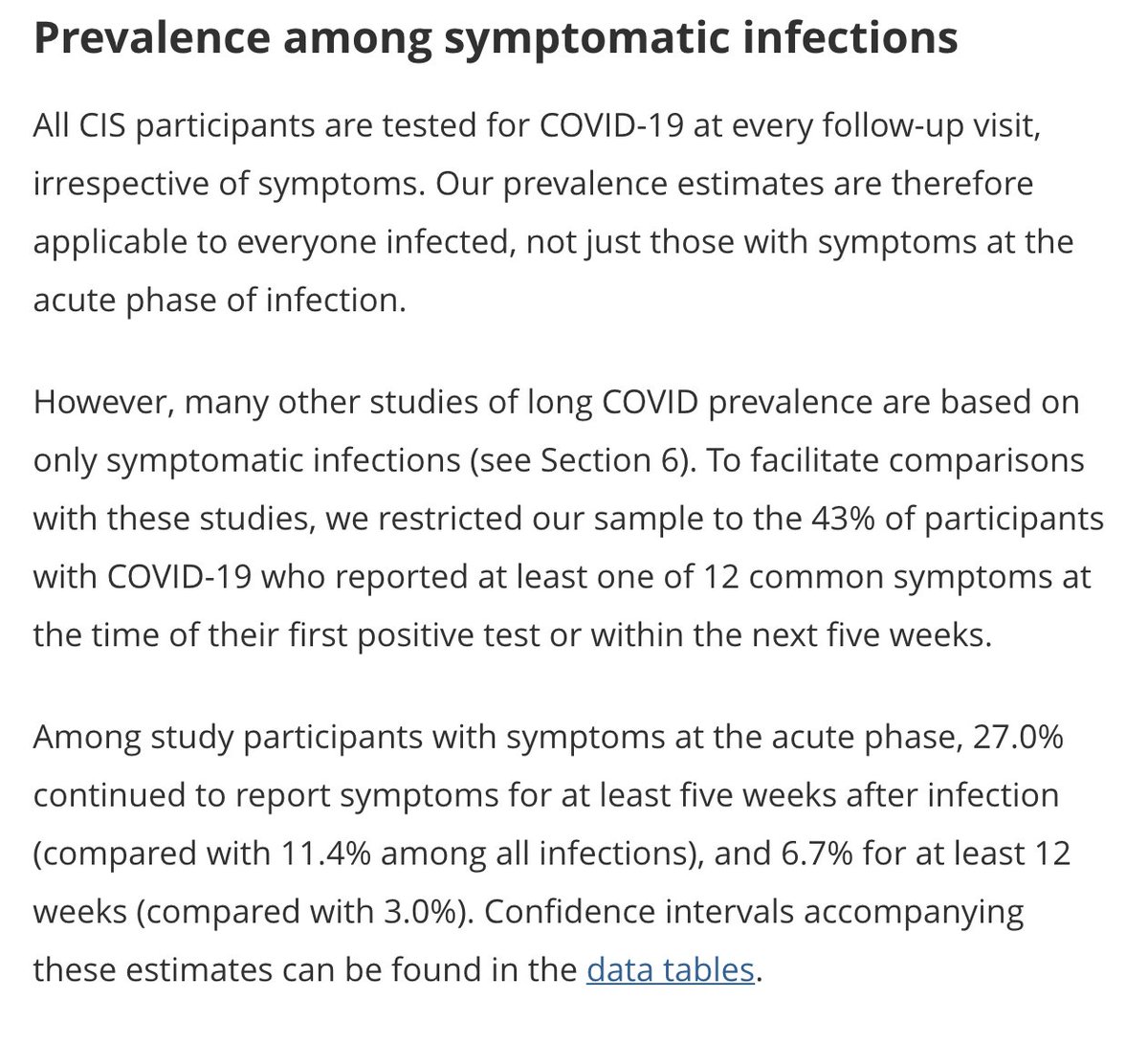
Also important to realise that ONS data includes both *asymptomatic* and *symptomatic* individuals, unlike other surveys that are based on cases that have tested positive for SARS-CoV-2 routinely, which is usually in people who are symptomatic.
When the ONS analysis is limited to symptomatic people (those who will generally be picked up due to testing in the acute illness), the prevalence more than *doubled* even with the 12 limited symptoms assessed. So increased from 11 to 27% at 5 wks and 3 to 7% at 12 weeks.
So what happens when you don't limit the analysis to 12 symptoms? The ONS also asked people to self report whether they felt they had had persistent long-term symptoms (without specifying the 12 or any others). Predictably, this gives higher estimates.


While these estimates are more likely to give a closer picture to reality, they may also be limited - because surveys have shown that we tend to underestimate if we don't ask for specific symptoms systematically.
Also worth remembering that several of the 12 symptoms may be quite hard to pick up in young kids, and questionnaires need modification to understand how young children may respond to post-covid symptoms. This may need more specialist assessment.
Also worth remembering that the ONS prevalence surveys that ask about self-reported persistent symptoms suggest 1 million of people in the population are currently living with this, 2/3rds of whom says it impacts their day to day lives. This is not trivial.
And in children, 11,000 children (or their parents) say they've had symptoms for more than 1 year after COVID-19. We don't need a control group to tell this is *not normal*.
And of course more and more evidence now that it isn't 'just symptoms', as if that were not enough... even people with mild disease go on to have reduction in renal function, thinning of grey matter in their brains 5-6 months after acute illness. So let's not trivialise this.
I'm frankly completely fed up with the BBCs takes on literally every long COVID study. Whether it is a study of >40 symptoms shows 1 in 7 kids being affected for 15 weeks, or is a limited study of 12 symptoms showing 3-10% of people affected, the message is always the same.
'this isn't as bad as we thought'.. let's remember that 30K people are being confirmed as cases every day (number of infections is likely *much* higher). Even if 'only' 5% of these people went on to get chronic symptoms that would be 1,500 *every single day*
So, is that reassuring?
Asking the BBC, and @apsmunro
Asking the BBC, and @apsmunro
And if anyone is interested in why the current ONS estimates are so different from the previous ones- this is an important question, which the authors of the report have explained really well. Report below if you'd like to delve further:
ons.gov.uk/peoplepopulati…
ons.gov.uk/peoplepopulati…
I also find it interesting (read troubling) that the same people who've spend months discussing vague non-specific limitations of the ONS survey are now hailing this as the definitive study of long COVID, despite methodology not having changed much!
• • •
Missing some Tweet in this thread? You can try to
force a refresh


