
No Tonsils Tuesday
If you're interested in reducing decision fatigue and improving the flow of the care of unwell children, this may be for you.
Read on (a thread)
#NoTonsilTuesday
If you're interested in reducing decision fatigue and improving the flow of the care of unwell children, this may be for you.
Read on (a thread)
#NoTonsilTuesday
2- This only works if you practice in a setting with a low prevalence of complications of streptococcal infection, for example the UK, US and many other countries.
If that's you, throat infection in children may be simpler than you've benn led to believe.
Next, some truths
If that's you, throat infection in children may be simpler than you've benn led to believe.
Next, some truths
3- Tonsillitis is a nonsense term. Upper respiratory tract infection (URTI) involves the tonsils. Having swollen or exudative tonsils is a non-specific finding.
It does not predict complications.
It does not predict complications.
4- It has always been a reasonable decision to not treat tonsillitis with antibiotics. That is why countless numbers of ethics committees have approved studies in which treatment of tonsillitis is compared to placebo and can continue to do so.
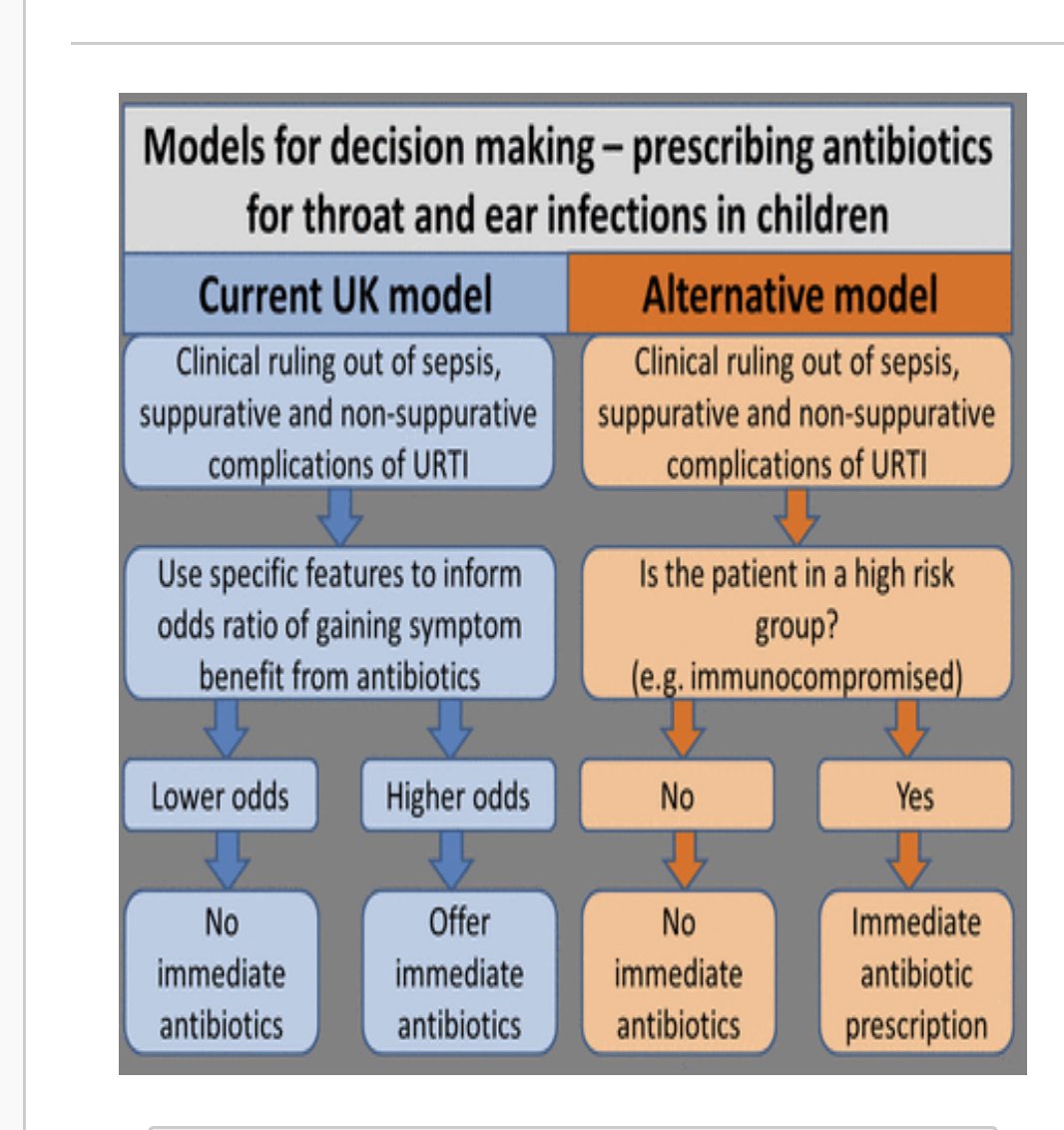
5- The real question in a child with URTI should always be "are there complications?" Complications such as abscess or glomerulonephitis are rare in most countries. When they are present that is a very different clinical scenario.
6- Symptom benefit and prevention of complications are either poor or non-existant in low prevalence countries. Side effect rates from antibiotics are high. As a result the benefit of antibiotics in the absence of complications is highly questionable in children.
7- There is therefore a strong argument for not looking at a child's throat when there are reasonable indicators (cough, coryza) of an URTI. If antibiotics are not the answer why look?
Further reading here: ep.bmj.com/content/edprac…
Further reading here: ep.bmj.com/content/edprac…
8- What about finding a focus? In most cases, a clinician is excluding significant focus. These include sepsis, meningitis and pneumonia. In fact, seeing swollen exudative tonsils rules none of these out and can be a distraction.
9- So how do these significant infections get ruled out? By looking at the child, their physiology and their breathing. Not by seeing their tonsils.

10- This is nothing new. Every parental decision to give symptomatic treatment to a febrile child does this. Every remote assessment is based on this.
It is also valid face to face.
As a bonus there's one fewer unpleasant procedure happening to children.
It is also valid face to face.
As a bonus there's one fewer unpleasant procedure happening to children.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



