What do currently active cases on Israeli MoH dashboard say about vaccine effectiveness vs. infection/severe disease for those vaccinated and with/without booster?
Here are the current data as of October 7, 2021 after roughly 2 months of delivery of boosters:
Here are the current data as of October 7, 2021 after roughly 2 months of delivery of boosters:

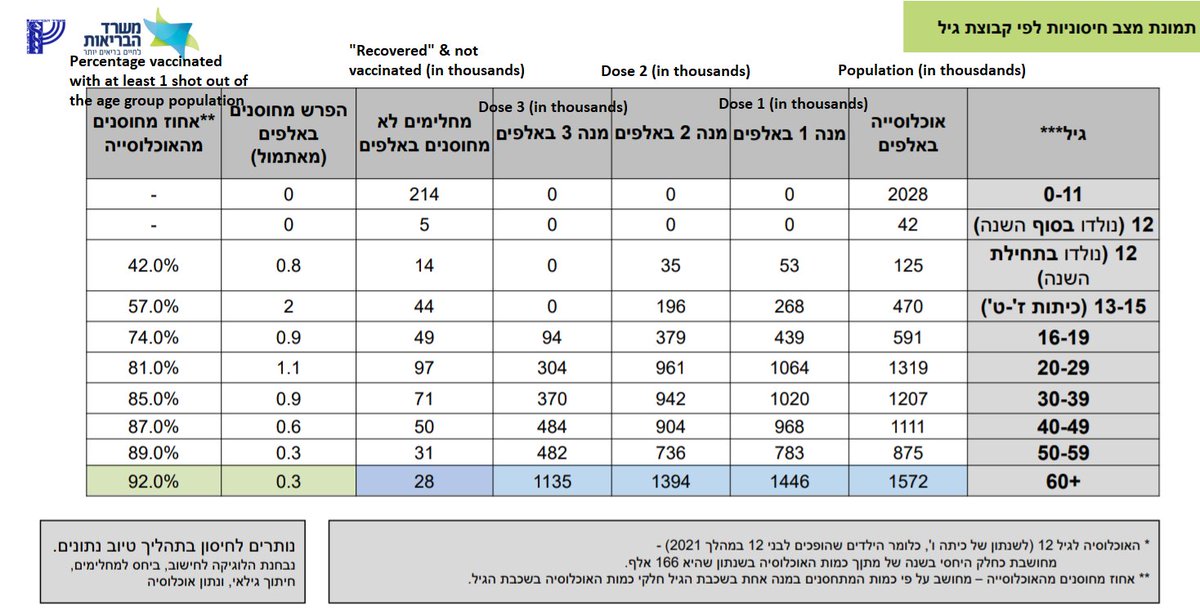
These data come from the Israel MoH dashboard from October 7, 2021 (datadashboard.health.gov.il/COVID-19/gener…) and include counts of currently active infections and severe infections by age group, split out by vaccination status (unvaccinated, boosters, or vaccinated but no boosters).
I simply computed "vaccine effectiveness" for vaccine (or booster) as the 1 minus the ratio of the infection (or serious infection) rate for the vaccinated (or boosted) group and the unvaccinated group.
Note that this is only a snapshot of current cases.
Note that this is only a snapshot of current cases.
We see that for infection, VE is only 50-60% for those not boosted, while for the boosted group it is ~90-95%. Boosters clearly restore the protection vs. infection that has been shown to wane over time.
However, we still see un-boosted vaccinated still retain substantial protection at 55-60%.
In September, we know >1/3 of 20-59 unvax population was previously infected, so these VE may be attenuated by the subset of unvax with strong immune protection.
covid-datascience.com/post/israeli-m…
In September, we know >1/3 of 20-59 unvax population was previously infected, so these VE may be attenuated by the subset of unvax with strong immune protection.
covid-datascience.com/post/israeli-m…
When we look at severe disease, we see even without boosters we see strong protection vs. severe disease in the vaccinated group that has not been boosted.
Of course the boosters top off that protection and push it near 100%
Of course the boosters top off that protection and push it near 100%
There is no question that boosters restore high levels of protection vs. infection and severe disease.
The question is whether they are necessary or desirable for all age groups, especially in the context of a long term strategy.
The question is whether they are necessary or desirable for all age groups, especially in the context of a long term strategy.
Is it reasonable to plan to give boosters every 4-6m into the future to maintain exceptionally high levels of neutralizing antibodies vs SARS-CoV-2 in our bloodstream?
Possibly, this makes sense during surges of the pandemic, but maybe not as a long term strategy.
Possibly, this makes sense during surges of the pandemic, but maybe not as a long term strategy.
Of course these simple VE estimates have limitations:
1. They are only based on a snapshot of "current" cases in Israel
2. While adjusting for age, they do not adjust for other confounders including co-morbidities, vaccination time, or sex/race and time infected.
1. They are only based on a snapshot of "current" cases in Israel
2. While adjusting for age, they do not adjust for other confounders including co-morbidities, vaccination time, or sex/race and time infected.
3. As mentioned, previous infection does not appear to be separated out of MoH data, & these comprise a substantial proportion of unvaccinated.
4. There may be other factors determining who got boosted or not, and these may also bias the VE.
I still find these data informative.
4. There may be other factors determining who got boosted or not, and these may also bias the VE.
I still find these data informative.
• • •
Missing some Tweet in this thread? You can try to
force a refresh