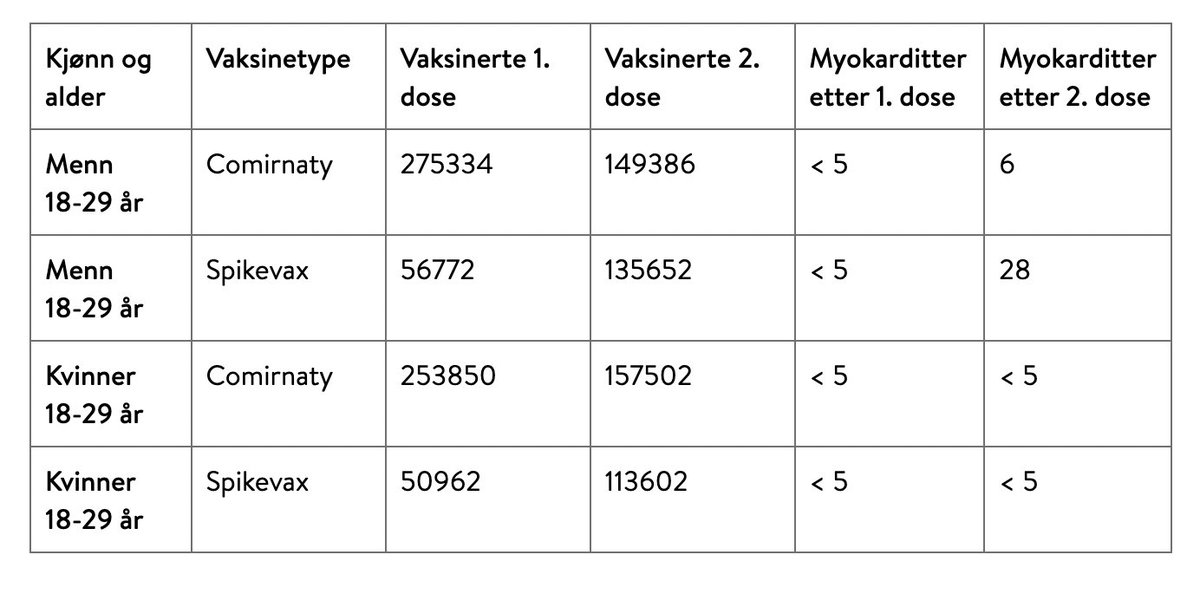
The Nordic data on the frequency of myocarditis after dose 2 of Moderna (Spikevax) in 18-29 year old men have been released: 1/4,800.
For Pfizer, it's 1/25,000.
fhi.no/nyheter/2021/m…
>5x difference, but see data from Ontario below (1/5)
For Pfizer, it's 1/25,000.
fhi.no/nyheter/2021/m…
>5x difference, but see data from Ontario below (1/5)
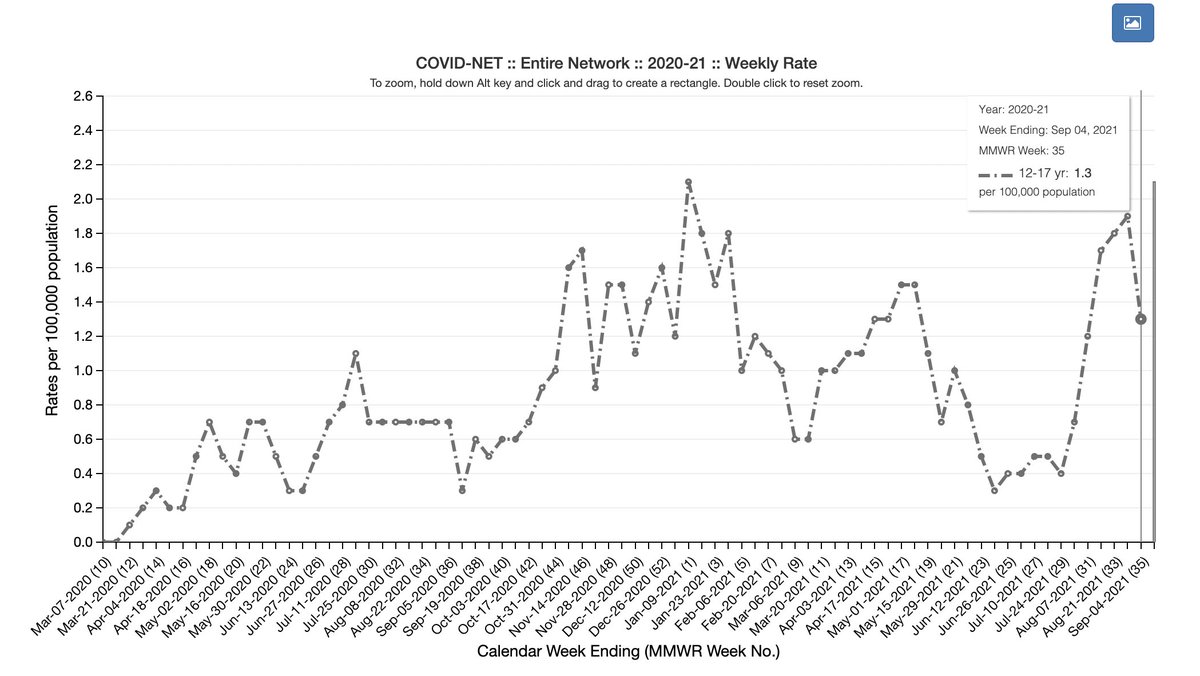
Ontario rate is now 1/5600 (mostly Pfizer) in boys 12-17
My ?: Is some of the increase in frequency simply due to awareness of condition? (in addition to increased Moderna use?) 2/5
My ?: Is some of the increase in frequency simply due to awareness of condition? (in addition to increased Moderna use?) 2/5
https://twitter.com/rubiconcapital_/status/1447704931767668738
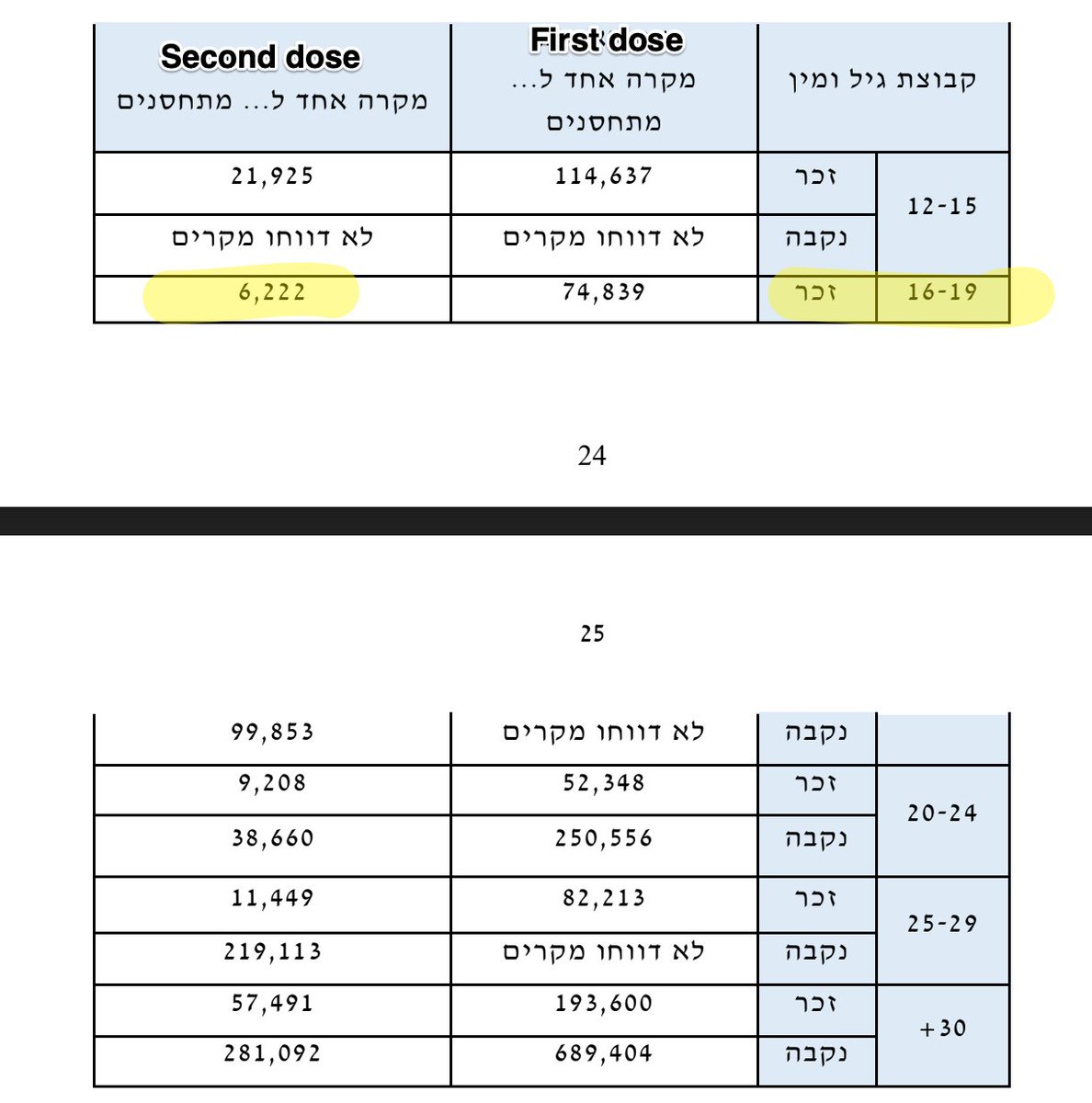
- Israel rate from NEJM 1/6600 for 16-19 yo (Pfizer) nejm.org/doi/full/10.10…
(For ref our VAERS pre-print: 1/6200 in 12-15 yo males, 1/10,600 in 16-17 yo (Pfizer))
Reports taken together point to ⬆️ rate in younger boys & after Moderna & ⬆️ awareness of this condition 3/5
(For ref our VAERS pre-print: 1/6200 in 12-15 yo males, 1/10,600 in 16-17 yo (Pfizer))
Reports taken together point to ⬆️ rate in younger boys & after Moderna & ⬆️ awareness of this condition 3/5
I keep saying this, but the question is: how do we minimize harm? One dose in some young males? Accept natural immunity, esp in young males? Decreased dosing? I don't have the answers but I think asking questions is important. 4/5
This condition seems mostly mild but not 100% of the time. Please listen to @drjohnm 's discussion of the severity seen in the recent Israeli papers in @NEJM . The point he makes about these mRNA vaccines being life saving is crucial. 5/5 podcasts.apple.com/us/podcast/thi…
• • •
Missing some Tweet in this thread? You can try to
force a refresh