#EACTS2021
Good morning everyone!
Spoilt for choice, unsure which session to attend but I am at Controversies in Transcatheter valve treatments
First talk is on TAVI in nonagenarians (>90 yrs old) - is there a survival benefit? by @RoxanneStL
Great and vital question!
Good morning everyone!
Spoilt for choice, unsure which session to attend but I am at Controversies in Transcatheter valve treatments
First talk is on TAVI in nonagenarians (>90 yrs old) - is there a survival benefit? by @RoxanneStL
Great and vital question!

#EACTS2021
If someone has already lived far past the average life expectancy in their country and is now into their 90s, can we *promise* the patient that TAVI will make them live longer?
In our centre, we feel that patients >90 need to be very motivated to have a procedure
If someone has already lived far past the average life expectancy in their country and is now into their 90s, can we *promise* the patient that TAVI will make them live longer?
In our centre, we feel that patients >90 need to be very motivated to have a procedure
#EACTS2021
Retrospective study looking at everyone age >90 that had TAVI & then matched them to the Quebec general population that are >90 years
Retrospective study looking at everyone age >90 that had TAVI & then matched them to the Quebec general population that are >90 years

#EACTS2021
I love it when we see tables like this and the presenter says "As you can see..." No, I can't see! 😆
75% Balloon-expandable THV
25% Self-expandable THV
Mortality 11/171 (6%); stroke 9/171 (5%); new LBBB 22/171 (13%)
I love it when we see tables like this and the presenter says "As you can see..." No, I can't see! 😆
75% Balloon-expandable THV
25% Self-expandable THV
Mortality 11/171 (6%); stroke 9/171 (5%); new LBBB 22/171 (13%)

#EACTS2021
Here are the univariable & multivariable Cox regression analyses & KM curve suggesting a significant survival advantage for those undergoing TAVI
Thought provoking...
Here are the univariable & multivariable Cox regression analyses & KM curve suggesting a significant survival advantage for those undergoing TAVI
Thought provoking...


#EACTS2021
So, the conclusion was that nonagenarians should not be denied TAVI on lack of prognostic benefit grounds
My thought is...what if high gradient severe AS but no symptoms? In our centre, an asymptomatic pt >90 would not get TAVI...what would you do in your hospital?
So, the conclusion was that nonagenarians should not be denied TAVI on lack of prognostic benefit grounds
My thought is...what if high gradient severe AS but no symptoms? In our centre, an asymptomatic pt >90 would not get TAVI...what would you do in your hospital?
#EACTS2021
Next talk from @Claudmuneretto on the important issue of patients with small aortic annuli - should they have a sutureless / rapid deployment valve or a TAVI?
@GilbertTangMD @mrjzacharias
Next talk from @Claudmuneretto on the important issue of patients with small aortic annuli - should they have a sutureless / rapid deployment valve or a TAVI?
@GilbertTangMD @mrjzacharias

#EACTS2021
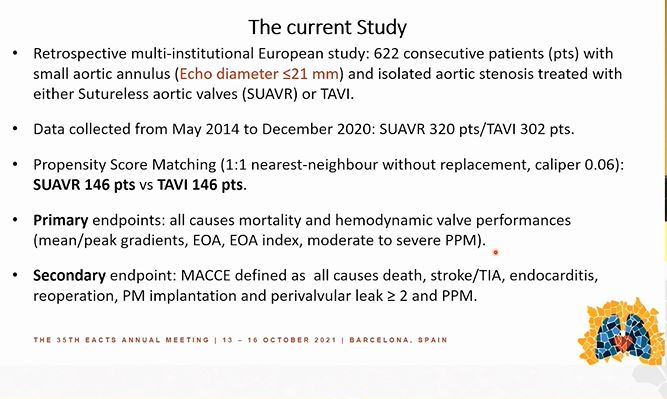
Starts by reminding us of the issues with small aortic annuli, including high risk of patient prosthesis mismatch
Starts by reminding us of the issues with small aortic annuli, including high risk of patient prosthesis mismatch


#EACTS2021
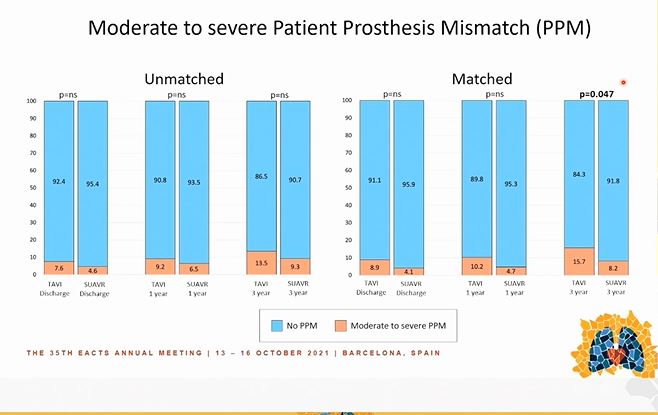
Less PVL & less need for pacemakers in patients with sutureless valves
After some statistical gymnastics (aka matching), there appears to be increased PPM with TAVI compared to sutureless valves also
Less PVL & less need for pacemakers in patients with sutureless valves
After some statistical gymnastics (aka matching), there appears to be increased PPM with TAVI compared to sutureless valves also


#EACTS2021
Conclusions - Sutureless bioprostheses may be superior to TAVI in these patients with small aortic annuli
So...what do I think? I think we need...a randomised study! Maybe one is already underway, I don't know...
Conclusions - Sutureless bioprostheses may be superior to TAVI in these patients with small aortic annuli
So...what do I think? I think we need...a randomised study! Maybe one is already underway, I don't know...

#EACTS2021
Next talk from @MMarinCuartas looking at outcomes when performing SAVR after a prior TAVI
Next talk from @MMarinCuartas looking at outcomes when performing SAVR after a prior TAVI

#EACTS2021
A single-centre retrospective analysis of 28 patients
Main reason for re-intervention was endocarditis - important to remember this, TAVI valves are biological valves and they get infected too, just like surgical bioprostheses
A single-centre retrospective analysis of 28 patients
Main reason for re-intervention was endocarditis - important to remember this, TAVI valves are biological valves and they get infected too, just like surgical bioprostheses


#EACTS2021
Median time from TAVI to AVR was just 7 months...I guess some of these valves may have had bacterial entry into the body at the time of the TAVI procedure?
Median time from TAVI to AVR was just 7 months...I guess some of these valves may have had bacterial entry into the body at the time of the TAVI procedure?





#EACTS2021
Conclusions
SAVR after TAVI is feasible, but (obviously) carries high risk.
The most common reason for repeat intervention is endocarditis
Conclusions
SAVR after TAVI is feasible, but (obviously) carries high risk.
The most common reason for repeat intervention is endocarditis

#EACTS2021
Next, an interesting talk from @JohannPetersen looking at physical & mental recovery after SAVR and TAVI
Next, an interesting talk from @JohannPetersen looking at physical & mental recovery after SAVR and TAVI


#EACTS2021
Mean age ~73-75yrs
Here are physical & mental recovery slides - I interpreted the 6MWT graph as this being greater for SAVR than TAVI? Unsure if y axis is change (delta) in 6MWT distance or absolute distance...
Mean age ~73-75yrs
Here are physical & mental recovery slides - I interpreted the 6MWT graph as this being greater for SAVR than TAVI? Unsure if y axis is change (delta) in 6MWT distance or absolute distance...




#EACTS2021
Next, a comparison of ProGlide versus surgical cutdown in TF TAVI from Dr Jan Rychter (Poland)
Next, a comparison of ProGlide versus surgical cutdown in TF TAVI from Dr Jan Rychter (Poland)

#EACTS2021
Here are the study objectives and their methodology - this is data from a national (POLTAVI) registry
As you can see, large numbers in each group
Here are the study objectives and their methodology - this is data from a national (POLTAVI) registry
As you can see, large numbers in each group


#EACTS2021
Mean age 79yrs
~20% have peripheral arterial disease
I missed the main results slide (!), here's the bleeding data
Mean age 79yrs
~20% have peripheral arterial disease
I missed the main results slide (!), here's the bleeding data


#EACTS2021
Must commend the speaker for including a limitations slide; very important to acknowledge this for these retrospective studies in which inevitably there will be biases that cannot be corrected, even by PSM!
Must commend the speaker for including a limitations slide; very important to acknowledge this for these retrospective studies in which inevitably there will be biases that cannot be corrected, even by PSM!



#EACTS2021
I think most of us have now moved over to LA rather than GA, certainly in most UK centres that is true
Still, here's their methods...
I think most of us have now moved over to LA rather than GA, certainly in most UK centres that is true
Still, here's their methods...

#EACTS2021
FELLOWS / RESIDENTS - please DON'T do this!
I understand there may be a limitation on number of slides and on time but...
what am I supposed to read from this?!
FELLOWS / RESIDENTS - please DON'T do this!
I understand there may be a limitation on number of slides and on time but...
what am I supposed to read from this?!


#EACTS2021
Here is their conclusion
In my hospital, we only use GA for the rare transapical case or for TF cases where surgical cut-down is needed or other reasons like patient would not tolerate sedation / LA approach
Here is their conclusion
In my hospital, we only use GA for the rare transapical case or for TF cases where surgical cut-down is needed or other reasons like patient would not tolerate sedation / LA approach

#EACTS2021
Final presentation on the Royal Brompton's experience using the Tendyne TMVI system - hope you saw my thread last night on the TMVI session, so you should be up to speed with what this is! 😀
@GilbertTangMD
Final presentation on the Royal Brompton's experience using the Tendyne TMVI system - hope you saw my thread last night on the TMVI session, so you should be up to speed with what this is! 😀
@GilbertTangMD

#EACTS2021
The Royal Brompton has a large experience with the Tendyne system, here we saw their data
The Royal Brompton has a large experience with the Tendyne system, here we saw their data

#EACTS2021
Retrospective analysis of their 26 patients that had a Tendyne procedure between 2014-2020
24/26 had secondary MR
Retrospective analysis of their 26 patients that had a Tendyne procedure between 2014-2020
24/26 had secondary MR


#EACTS2021
Here are their results...
Significant reduction in PA pressures, no change in LV cavity size or LV EF
Improvement in NYHA status
Here are their results...
Significant reduction in PA pressures, no change in LV cavity size or LV EF
Improvement in NYHA status



#EACTS2021
52% survival at 3yrs; some patients died last year due to COVID-19 (may still be alive otherwise)
For patients that cannot have surgery or TEER, I think these are encouraging results...
52% survival at 3yrs; some patients died last year due to COVID-19 (may still be alive otherwise)
For patients that cannot have surgery or TEER, I think these are encouraging results...

• • •
Missing some Tweet in this thread? You can try to
force a refresh