#EACTS2021
Dr Alfieri reminded us that medicine has a long history of collaboration between different specialties and areas of science/engineering
He gave the example of Lowell Edwards (engineer) & Albert Starr (surgeon) to create the ball-in-cage valve - same for Bjork-Shiley
Dr Alfieri reminded us that medicine has a long history of collaboration between different specialties and areas of science/engineering
He gave the example of Lowell Edwards (engineer) & Albert Starr (surgeon) to create the ball-in-cage valve - same for Bjork-Shiley

#EACTS2021
Why do we have a Heart Team?
Dr Alfieri highlighted this can broadly be divided into these three categories. I really like this...
Why do we have a Heart Team?
Dr Alfieri highlighted this can broadly be divided into these three categories. I really like this...

#EACTS2021
He used ischaemic cardiomyopathy as a great example of increasing complexity of the disease...and thus the wide number of skill sets required
He used ischaemic cardiomyopathy as a great example of increasing complexity of the disease...and thus the wide number of skill sets required


#EACTS2021
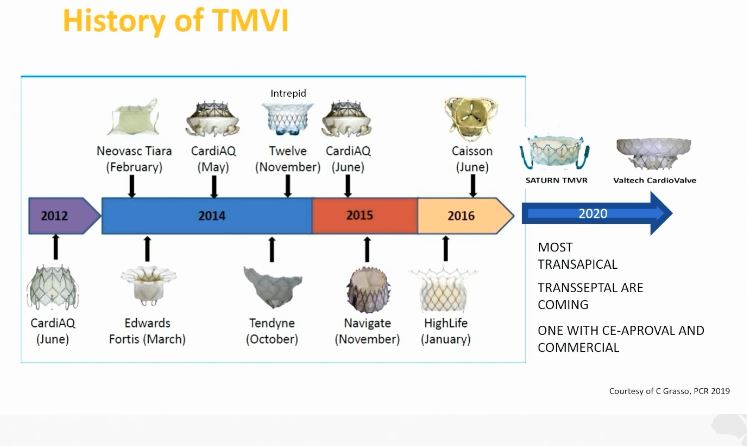
This is the 3rd dimension - increasing array of therapeutic options for patients. He highlighted the multitude of options for aortic & mitral valve interventions available today
This is the 3rd dimension - increasing array of therapeutic options for patients. He highlighted the multitude of options for aortic & mitral valve interventions available today

#EACTS2021
Are there potential downsides to this approach? Yes.
I really liked this SWOT analysis (Strengths; Weaknesses; Opportunities; Threats) that he presented
Are there potential downsides to this approach? Yes.
I really liked this SWOT analysis (Strengths; Weaknesses; Opportunities; Threats) that he presented

#EACTS2021
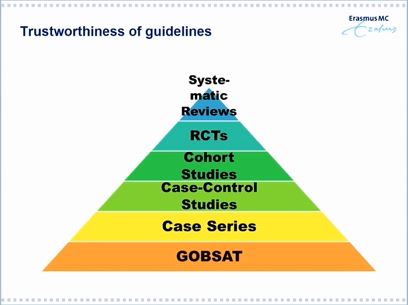
Next was a presentation by former ESC President and multi-modality cardiac imager Dr Jeroen Bax, who discussed the role and place of the Heart Team in the guidelines
Next was a presentation by former ESC President and multi-modality cardiac imager Dr Jeroen Bax, who discussed the role and place of the Heart Team in the guidelines



#EACTS2021
Dr Bax explained the changes between the 2017 & 2021 ESC guidelines on VHD...explaining the reasons for including Heart Team discussions - usually for the most complex cases or ones in which several treatment options exist
Dr Bax explained the changes between the 2017 & 2021 ESC guidelines on VHD...explaining the reasons for including Heart Team discussions - usually for the most complex cases or ones in which several treatment options exist

#EACTS2021
A great flowchart showing the flow of care between networks
Last year, the @BrHeartValveSoc produced its Blueprint which discussed the importance of network-based care. Not all hospitals / centres have all options and expertise - and they don't all need to!
A great flowchart showing the flow of care between networks
Last year, the @BrHeartValveSoc produced its Blueprint which discussed the importance of network-based care. Not all hospitals / centres have all options and expertise - and they don't all need to!

#EACTS2021
A great question - does *every* patient need to be discussed by the Heart Team, even where the decision is clear?
Dr Bax was clear the answer is NO - the Heart Team should be reserved for more complex cases. I agree. Most Heart Teams would not have time to do this
A great question - does *every* patient need to be discussed by the Heart Team, even where the decision is clear?
Dr Bax was clear the answer is NO - the Heart Team should be reserved for more complex cases. I agree. Most Heart Teams would not have time to do this
#EACTS2021
Next talk from Dr Hendrik Treede on potential threats to the Heart Team approach - especially cost
Next talk from Dr Hendrik Treede on potential threats to the Heart Team approach - especially cost
#EACTS2021
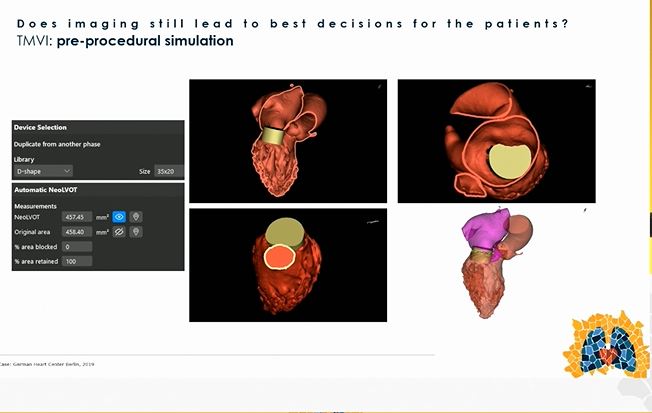
Then a very interesting talk (for me!) on whether imaging still leads to best decisions for patients - pleased to hear early on a resounding Yes from Dr Unbehaun!
Then a very interesting talk (for me!) on whether imaging still leads to best decisions for patients - pleased to hear early on a resounding Yes from Dr Unbehaun!

#EACTS2021
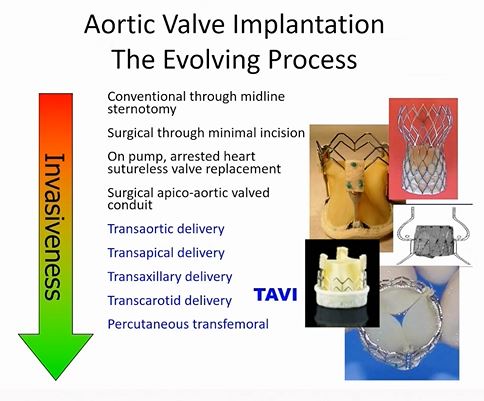
As minimally invasive and transcatheter procedures have increased, so has the need for 3D imaging to plan successful procedures
As minimally invasive and transcatheter procedures have increased, so has the need for 3D imaging to plan successful procedures


#EACTS2021
Love these slides. Not only can imaging tell you if the procedure can be done, but also how hard it might be and what precautions might be needed.
Indeed, TAVI or TMVI without high quality imaging are impossible!
@AusamiAbbas
Love these slides. Not only can imaging tell you if the procedure can be done, but also how hard it might be and what precautions might be needed.
Indeed, TAVI or TMVI without high quality imaging are impossible!
@AusamiAbbas

#EACTS2021
Great example relating to V-in-V TAVI...imaging can tell you likelihood of coronary obstruction and thus whether the #BASILICA technique will be required
True!
Great example relating to V-in-V TAVI...imaging can tell you likelihood of coronary obstruction and thus whether the #BASILICA technique will be required
True!

#EACTS2021
Final talk by @PeymanSardari on Education in Cardiac Surgery and the role of the Heart Team
Great first slide. Everyone loves Santa...but Santa does not exist...same for the Heart Team! 😆
Final talk by @PeymanSardari on Education in Cardiac Surgery and the role of the Heart Team
Great first slide. Everyone loves Santa...but Santa does not exist...same for the Heart Team! 😆

#EACTS2021
Over 70 transcatheter devices on the market; none suitable for all patients...and no Dr can be expert in all of these...so, have to select the right device for the right patient to be done by right operator(s) in the right centre...and that'll need a Heart Team
Over 70 transcatheter devices on the market; none suitable for all patients...and no Dr can be expert in all of these...so, have to select the right device for the right patient to be done by right operator(s) in the right centre...and that'll need a Heart Team

#EACTS2021
Important points on this slide
Patient CoI referred to patients having done internet searches & coming to clinic with treatment plans already in place
It's a delicate balance; we should encourage patient empowerment and increasing their knowledge
Important points on this slide
Patient CoI referred to patients having done internet searches & coming to clinic with treatment plans already in place
It's a delicate balance; we should encourage patient empowerment and increasing their knowledge

#EACTS2021
"A successful episode of patient care is more than just them surviving the operation"
Dr Sardari Nia invited all to join the Heart Team Academy - a global effort to advance the field
Very true
"A successful episode of patient care is more than just them surviving the operation"
Dr Sardari Nia invited all to join the Heart Team Academy - a global effort to advance the field
Very true


#EACTS2021
What a superb final slide...love this!
Great session...hope you enjoyed this thread...more later!
What a superb final slide...love this!
Great session...hope you enjoyed this thread...more later!

• • •
Missing some Tweet in this thread? You can try to
force a refresh