/the information dilemma_
A 17-tweet summary of my academic contribution to the #KidneyWk 2021 meeting.
@ASNKidney: Thanks for selecting my work for presentation...I appreciate it.
A 17-tweet summary of my academic contribution to the #KidneyWk 2021 meeting.
@ASNKidney: Thanks for selecting my work for presentation...I appreciate it.

2
My disclosures
I am a physician-programmer. I analyze #SoMe data, with a keen focus on Twitter. I primarily analyze tweets in #NephTwitter and #CardioTwitter, and I have analyzed tweets for Oncology and Endocrinology organizations as well.
My disclosures
I am a physician-programmer. I analyze #SoMe data, with a keen focus on Twitter. I primarily analyze tweets in #NephTwitter and #CardioTwitter, and I have analyzed tweets for Oncology and Endocrinology organizations as well.

3
We face an information dilemma we face in medical communities. The dilemma originates from customized search results. How can anything customized *to/for you* be a negative?
It's negative when ≥2 people are searching for the same thing (the truth) & getting different results.
We face an information dilemma we face in medical communities. The dilemma originates from customized search results. How can anything customized *to/for you* be a negative?
It's negative when ≥2 people are searching for the same thing (the truth) & getting different results.

4
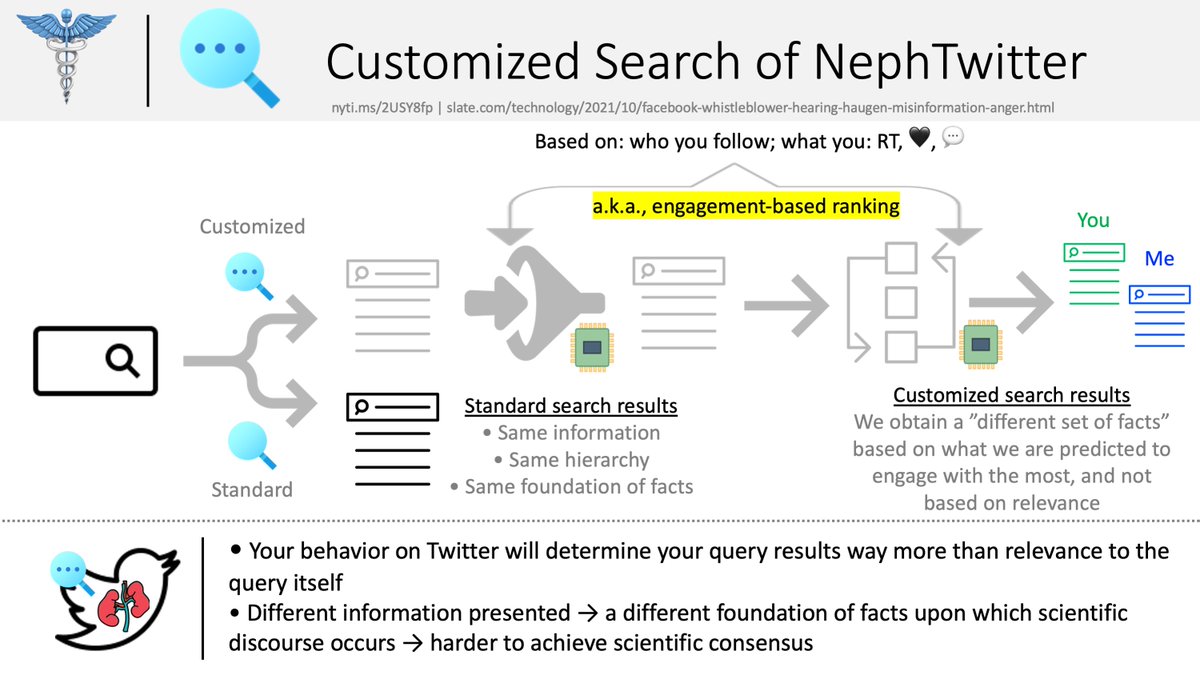
The schematic below shows the difference between standard and customized search. In the former, your search results are based exclusively on their relevance to your query. If ≥2 people make the same query, they get 1) the same results in 2) the same hierarchical order.
The schematic below shows the difference between standard and customized search. In the former, your search results are based exclusively on their relevance to your query. If ≥2 people make the same query, they get 1) the same results in 2) the same hierarchical order.

5
In customized search, the results are not based exclusively on their pertinence to your query. The results are a) filtered and b) reshuffled. In the end, ≥2 people who make an identical query will be presented with different search results in a different hierarchical order.
In customized search, the results are not based exclusively on their pertinence to your query. The results are a) filtered and b) reshuffled. In the end, ≥2 people who make an identical query will be presented with different search results in a different hierarchical order.

6
Why does this happen? Because results are shown to you based on what an algorithm predicts you will *engage* with the most. Customized search uses *engagement-based ranking* to present results in a particular order to you. Your pattern of RTs ❤️👍💭 determines...
Why does this happen? Because results are shown to you based on what an algorithm predicts you will *engage* with the most. Customized search uses *engagement-based ranking* to present results in a particular order to you. Your pattern of RTs ❤️👍💭 determines...

7
...what results you see & the order in which you see them. The results you see aren't presented to you because of their relevance to your search query, but rather because they are highly predicted to stimulate engagement from you.
...what results you see & the order in which you see them. The results you see aren't presented to you because of their relevance to your search query, but rather because they are highly predicted to stimulate engagement from you.
8
Naturally, ≥2 people making an identical query will be shown 2 sets of results in a unique order. Repeat this scenario over-and-over and you create groups of people who possess *a different* set of facts. Customized search results is the fuel for the developing the above.
Naturally, ≥2 people making an identical query will be shown 2 sets of results in a unique order. Repeat this scenario over-and-over and you create groups of people who possess *a different* set of facts. Customized search results is the fuel for the developing the above.
9
Here are 2 experiments that I conducted (you can as well). These are 2 Twitter accounts owned by me. I made an identical search query in both accounts: on the same date, minutes apart, from the same location, and using the same device.
Here are 2 experiments that I conducted (you can as well). These are 2 Twitter accounts owned by me. I made an identical search query in both accounts: on the same date, minutes apart, from the same location, and using the same device.


10
I received different results in a different order. This shouldn't happen. And although I am displaying the first 3 search results, I can drag this out to the first 25-35 results and the outcome is the same: different search results presented in a different hierarchical order.
I received different results in a different order. This shouldn't happen. And although I am displaying the first 3 search results, I can drag this out to the first 25-35 results and the outcome is the same: different search results presented in a different hierarchical order.


11
How do we mitigate the perils of customized search?
Contrary to popular belief, the solution to this pollution is not dilution. You cannot defeat the negative effects of an algorithm(s) by using brute human force and create quality/reliable/accurate medical content.
How do we mitigate the perils of customized search?
Contrary to popular belief, the solution to this pollution is not dilution. You cannot defeat the negative effects of an algorithm(s) by using brute human force and create quality/reliable/accurate medical content.

12
In the battle of human effort versus algorithm efficiency, the latter will win.
Every. Single. Time.
We need to write our own algorithms that restore search back to the standardized form.
This Superman III reference is apropos:
In the battle of human effort versus algorithm efficiency, the latter will win.
Every. Single. Time.
We need to write our own algorithms that restore search back to the standardized form.
This Superman III reference is apropos:

13
So I did. After 24 months of learning how to program a search engine and sitting on a wealth of #NephTwitter and #CardioTwitter scientific tweets from 2011, I created NephTwitterArchive.com. It is a search engine that *doesn't* collect any of your data.
So I did. After 24 months of learning how to program a search engine and sitting on a wealth of #NephTwitter and #CardioTwitter scientific tweets from 2011, I created NephTwitterArchive.com. It is a search engine that *doesn't* collect any of your data.

14
NephTwitterArchive.com translates all scientific tweets into English. It is agnostic to who you are and how you interact with content. Results are displayed based only on pertinence to your query. It's free without any ads or sponsors.
NephTwitterArchive.com translates all scientific tweets into English. It is agnostic to who you are and how you interact with content. Results are displayed based only on pertinence to your query. It's free without any ads or sponsors.

15
I launched it in 10/2019 without any advertising or 3rd-party promotion. From 10/2019-9/2021, a total of 37K searches have been completed. A *completed search* has a strict definition (see image).
I launched it in 10/2019 without any advertising or 3rd-party promotion. From 10/2019-9/2021, a total of 37K searches have been completed. A *completed search* has a strict definition (see image).

16
Interestingly, 42% of users visited NephTwitterArchive.com immediately *after* visiting Twitter or Facebook. Perhaps they didn't find what they were looking for on those platforms. Perhaps they knew/had a feeling that the results they were seeing wasn't the whole picture.
Interestingly, 42% of users visited NephTwitterArchive.com immediately *after* visiting Twitter or Facebook. Perhaps they didn't find what they were looking for on those platforms. Perhaps they knew/had a feeling that the results they were seeing wasn't the whole picture.

17
In conclusion, place a value on standardized search when it comes to finding scientific truth. Don't trust customized search engines in their entirety. Cross-reference search results from #SoMe platforms with NephTwitterArchive.com to be sure you have the full picture.
In conclusion, place a value on standardized search when it comes to finding scientific truth. Don't trust customized search engines in their entirety. Cross-reference search results from #SoMe platforms with NephTwitterArchive.com to be sure you have the full picture.

• • •
Missing some Tweet in this thread? You can try to
force a refresh