We published today a study on acute hypertension hospitalization trends, led by @yuan_lu1 and news is not good. Over last 20 yrs rates markedly increased even though this can be prevented w/simple & inexpensive strategies. ahajournals.org/doi/10.1161/CI… @YaleMed @YaleCardiology @CircAHA 

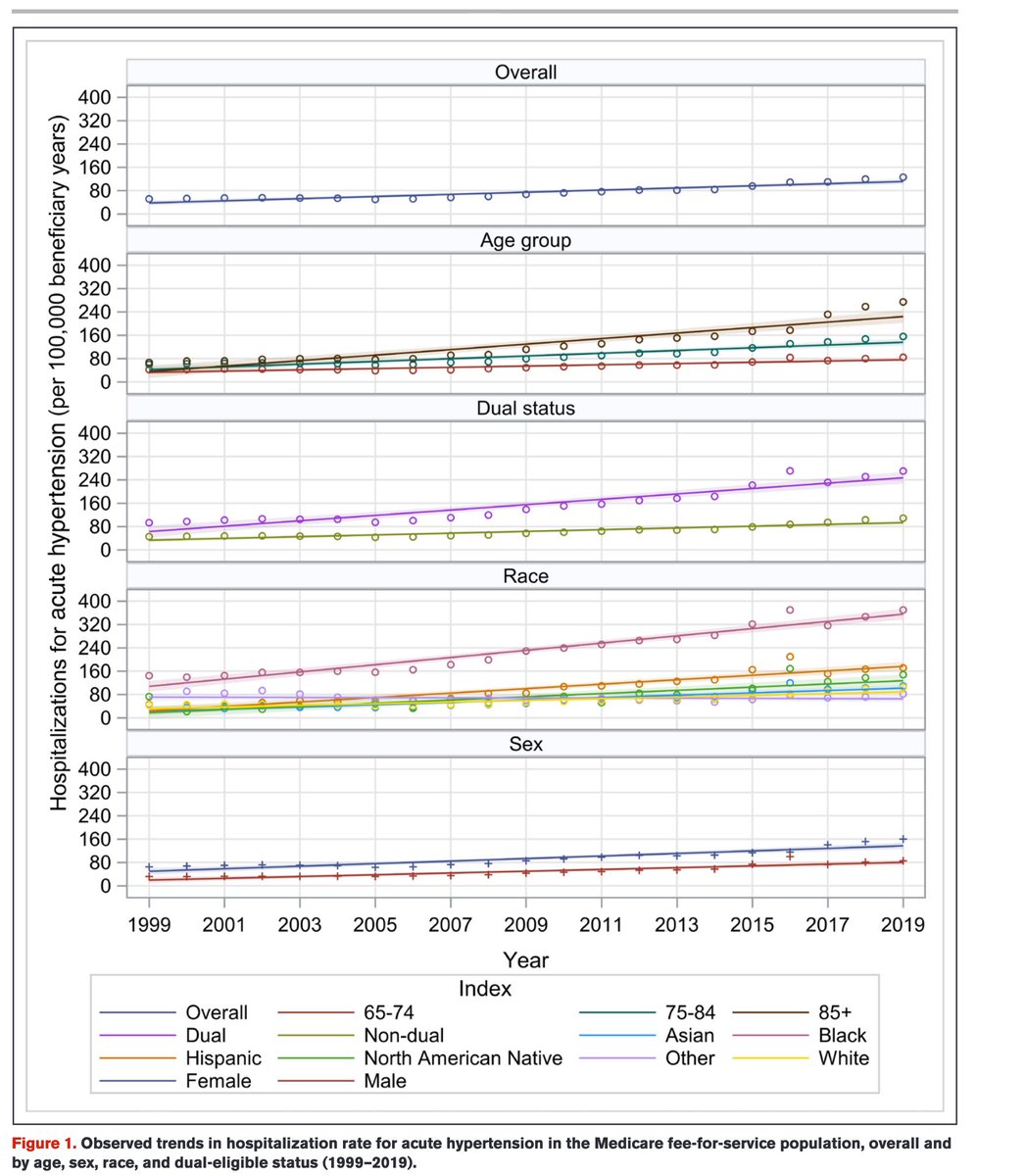
@yuan_lu1 @YaleMed @YaleCardiology @CircAHA And disappointingly but not surprisingly, the highest rates of acute hypertension hospitalizations were among Black patients, who also experienced the steepest increase over last 20 years. The hypertension crisis is also a health equity crisis. @AHAScience

@yuan_lu1 @YaleMed @YaleCardiology @CircAHA @AHAScience The increase in acute hypertension hospitalizations occurred in all subgroups. Makes sense since hypertension control is worse over time; hypertension deaths are rising. This must be recognized as a national crisis. @JeromeAdamsMD saw this as Surgeon General. This work is so imp.
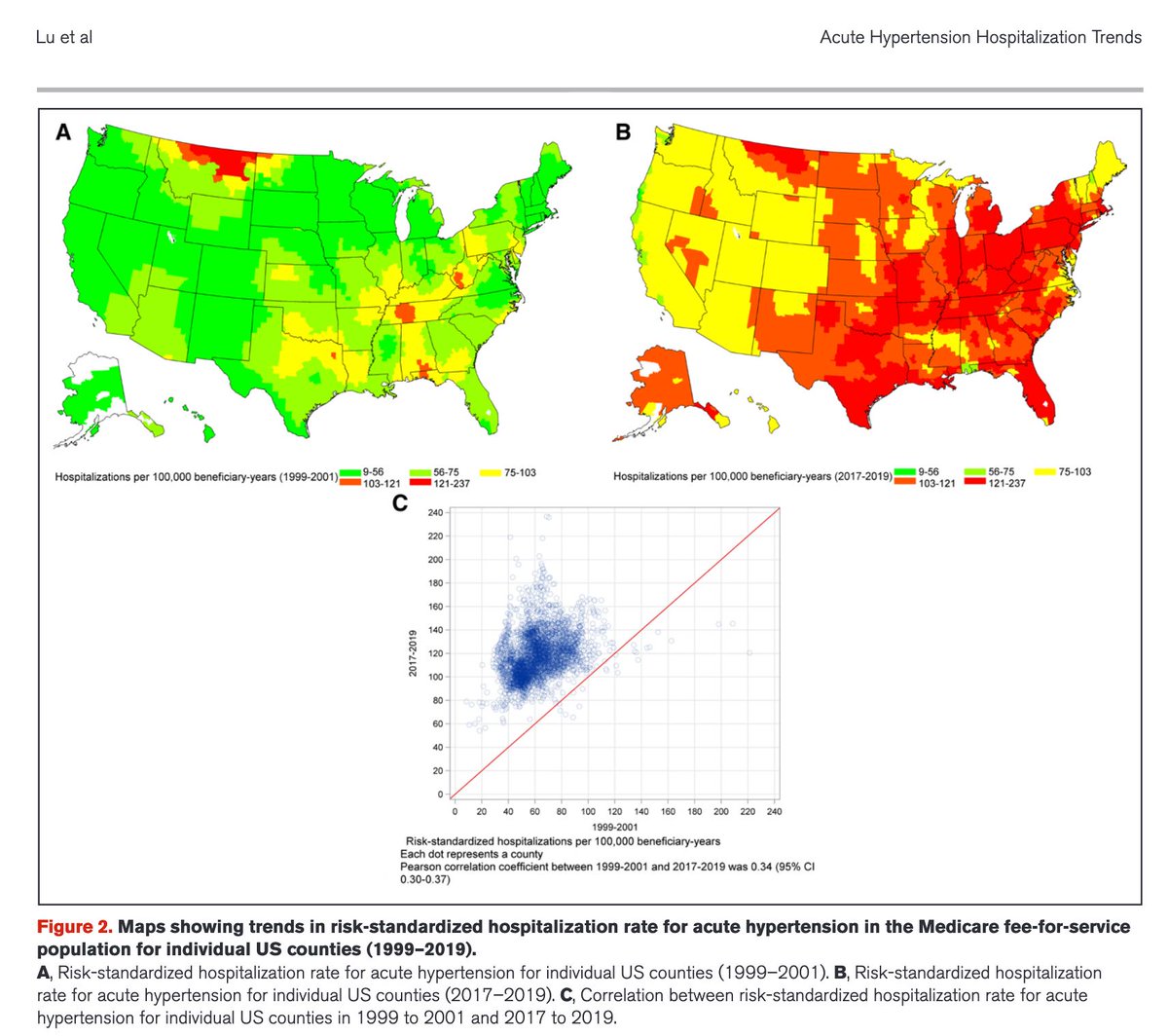
@yuan_lu1 @YaleMed @YaleCardiology @CircAHA @AHAScience @JeromeAdamsMD Take a look at how the map of the US has changed in the rates of acute hypertension hospitalizations; this is not sleight of hand with graphics. Hypertension causes terrible mortality and morbidity. We are losing the battle, even though we have effective treatments.
@yuan_lu1 @YaleMed @YaleCardiology @CircAHA @AHAScience @JeromeAdamsMD This study gives us even greater resolve to dedicate ourselves to reducing risk for people and populations by getting ahead of hypertension. It is a non-communicable disease pandemic.
@yuan_lu1 @YaleMed @YaleCardiology @CircAHA @AHAScience @JeromeAdamsMD Kudos to @yuan_lu1 for leading this study and for the cast of star co-authors: @kewatson @Fatimarodguez @FaRodriguezMD @SpatzErica @khurramn1 @oyi_kk - great teamwork. Just the beginning.
• • •
Missing some Tweet in this thread? You can try to
force a refresh