There’s a new SARS-CoV-2 variant of concern: Omicron (aka B.1.1.529) #OmicronVariant
What is this Omicron COVID variant & is the panic of it justified? (spoiler alert: no)
A short #OmicronExplainer 🧵 about what we actually know, what we suspect, & what’s still unknown.
1/
What is this Omicron COVID variant & is the panic of it justified? (spoiler alert: no)
A short #OmicronExplainer 🧵 about what we actually know, what we suspect, & what’s still unknown.
1/




4 reasons Omicron is worrisome:
1️⃣ it is spreading rapidly in South Africa (known)
2️⃣ it is highly mutated (known)
3️⃣some mutations likely increase transmissibility (suspected)
4️⃣others *may* allow it to evade existing immunity or vaccines (unknown)
We’ll talk about all 4...
2/
1️⃣ it is spreading rapidly in South Africa (known)
2️⃣ it is highly mutated (known)
3️⃣some mutations likely increase transmissibility (suspected)
4️⃣others *may* allow it to evade existing immunity or vaccines (unknown)
We’ll talk about all 4...
2/
First some nomenclature:
B.1.1.529 (its Pango lineage) is the same as “Omicron" (WHO declared it a variant of concern & assigned a Greek letter) #OmicronVariant
It’s also known as K21 (Nextstrain clade)
It’s erroneously been called the #NuVariant ... yeah that’s not a thing
3/
B.1.1.529 (its Pango lineage) is the same as “Omicron" (WHO declared it a variant of concern & assigned a Greek letter) #OmicronVariant
It’s also known as K21 (Nextstrain clade)
It’s erroneously been called the #NuVariant ... yeah that’s not a thing
3/



A while ago, genomic surveillance (sequencing the complete virus genome) identified a variant (designated K21) in South Africa.
Recently, this variant appears to have acquired many more mutations & become a (more) dominant strain in South Africa.
nextstrain.org/ncov/gisaid/af…
4/
Recently, this variant appears to have acquired many more mutations & become a (more) dominant strain in South Africa.
nextstrain.org/ncov/gisaid/af…
4/



Depending on the country, only a small % of COVID cases get sequenced.
Even though we only identify a fraction of the Omicron cases, we can extrapolate that Omicron is outcompeting Delta & becoming dominant in Africa.
(btw, this shows why collaborations like GSAID are 🔑)
5/
Even though we only identify a fraction of the Omicron cases, we can extrapolate that Omicron is outcompeting Delta & becoming dominant in Africa.
(btw, this shows why collaborations like GSAID are 🔑)
5/

As of today Saturday 11/27, there are 104 confirmed Omicron cases
Most (100) in 🇿🇦 South Africa & 🇧🇼 Botswana &
🇬🇧 2 in the UK
🇭🇰 2 in Hong Kong
🇮🇱 1 in Israel (+2 suspected)
🇧🇪 1 in Belgium
+ suspected cases in 🇨🇿 & 🇩🇪
Bookmark the GISAID dashboard
gisaid.org/hcov19-variant…
6/
Most (100) in 🇿🇦 South Africa & 🇧🇼 Botswana &
🇬🇧 2 in the UK
🇭🇰 2 in Hong Kong
🇮🇱 1 in Israel (+2 suspected)
🇧🇪 1 in Belgium
+ suspected cases in 🇨🇿 & 🇩🇪
Bookmark the GISAID dashboard
gisaid.org/hcov19-variant…
6/

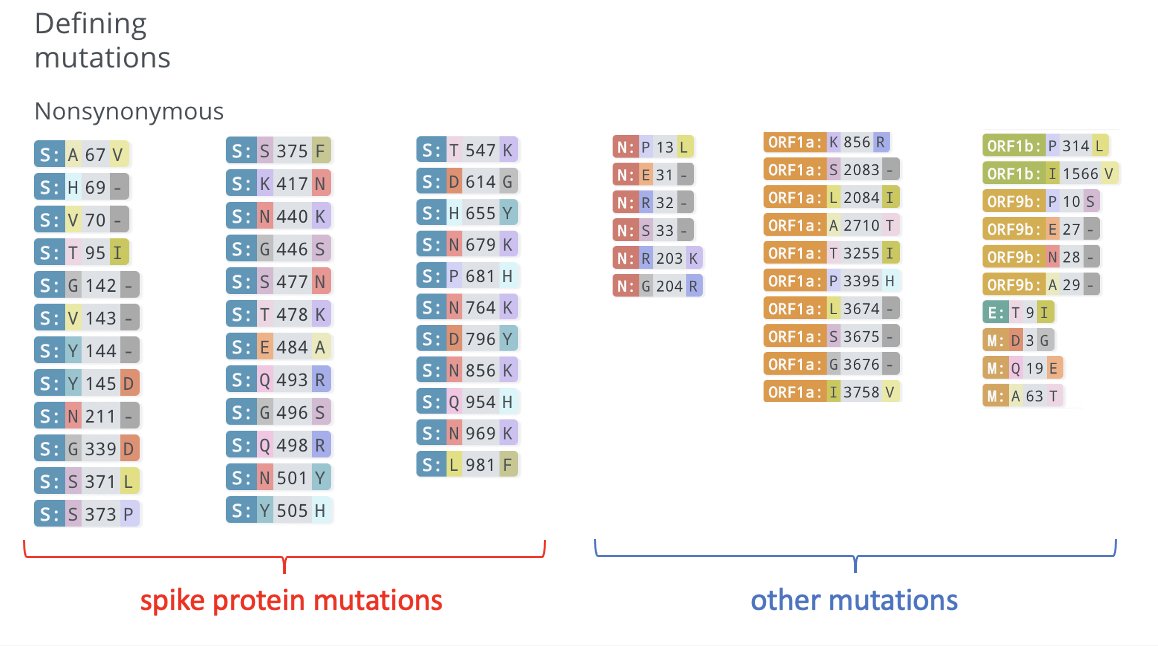
What *are* the defining mutations in Omicron?
There are a lot. Some we’ve seen before, a few are novel.
In total there are (at least) 35 mutations in the spike protein & 26 more in other genes.
There’s a great summary on covariants.org/variants/21K
7/
There are a lot. Some we’ve seen before, a few are novel.
In total there are (at least) 35 mutations in the spike protein & 26 more in other genes.
There’s a great summary on covariants.org/variants/21K
7/

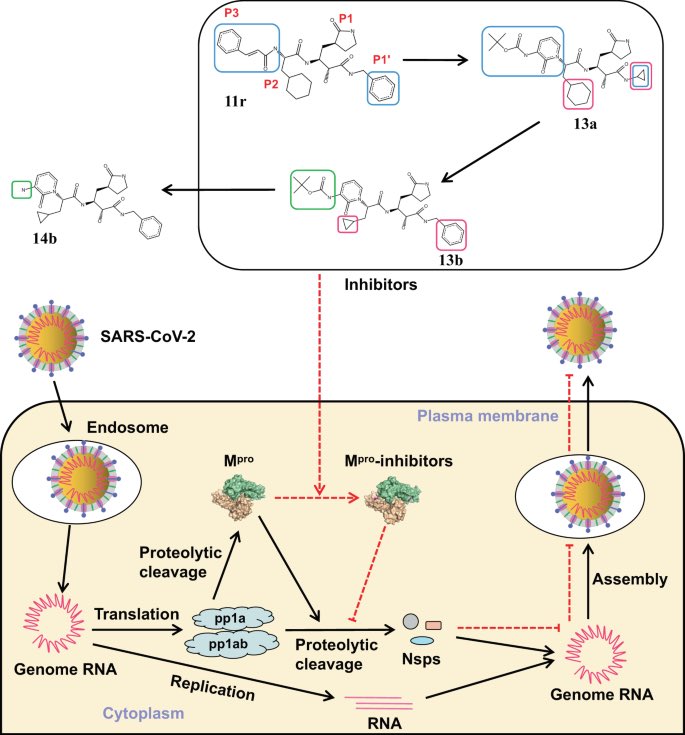
What's the significance of these mutations?
Several (orange) are in the region that binds to ACE2 (green ribbon); based on in vitro studies these may increase transmissibility
Similarly mutations at furin cleavage sites (H655Y, N679K, P681H) may also increase transmisibility
8/
Several (orange) are in the region that binds to ACE2 (green ribbon); based on in vitro studies these may increase transmissibility
Similarly mutations at furin cleavage sites (H655Y, N679K, P681H) may also increase transmisibility
8/
⚠️Notably, despite a lot of speculation about the “heavily mutated Omicron strain” there is no actual evidence that any of these mutations enables Omicron to evade vaccines.
Computational models are great but we will learn a lot in the coming weeks with in vitro studies.
9/
Computational models are great but we will learn a lot in the coming weeks with in vitro studies.
9/
Also important, the emergence of novel variants is an eventuality that governments & vaccine makers have prepared for.
One of the advantages of mRNA vaccines is that it's comparatively easier/faster to iterate *if* necessary,
Great summary of this👇
10/
One of the advantages of mRNA vaccines is that it's comparatively easier/faster to iterate *if* necessary,
Great summary of this👇
https://twitter.com/megtirrell/status/1464225637590310938?s=20
10/
Also important to remember that although the vaccines DO reduce the risk of infection & transmission, their big benefit is reducing the risk of serious illness or death.
While there are reports of Omicron breakthrough cases there are NO reports of serious illness/death (yet)
11/
While there are reports of Omicron breakthrough cases there are NO reports of serious illness/death (yet)
11/
Does Omicron differ clinically from Delta?
If it's hard to predict immune evasion from genome sequences its even harder to predict clinical course.
With ~100 confirmed cases, we know little about whether the clinical course of Omicron differs from other strains. (an unknown)
12/
If it's hard to predict immune evasion from genome sequences its even harder to predict clinical course.
With ~100 confirmed cases, we know little about whether the clinical course of Omicron differs from other strains. (an unknown)
12/
A lot of people are talking about this statement by the head of South Africa's medical association, claiming that Omicon causes "milder symptoms"
I view this skeptically.
I think it's too early to know how/if Omicron differs from Delta clinically.
13/
timesofindia.indiatimes.com/world/rest-of-…
I view this skeptically.
I think it's too early to know how/if Omicron differs from Delta clinically.
13/
timesofindia.indiatimes.com/world/rest-of-…
To summarize:
-Omicron (B.1.1.529) is a new SARS-CoV-2 variant of concern (known)
-there are a few cases outside of Africa (known)
-Omicron has many mutations (known) & some likely enhance transmission (suspected)
-So far, there is no evidence of vaccine evasion (an unknown)
14/
-Omicron (B.1.1.529) is a new SARS-CoV-2 variant of concern (known)
-there are a few cases outside of Africa (known)
-Omicron has many mutations (known) & some likely enhance transmission (suspected)
-So far, there is no evidence of vaccine evasion (an unknown)
14/
Should we worry? YES
A more infectious variant is very concerning, particularly when so much of the world remains unvaccinated.
But should we panic (as the markets did yesterday)? NO
There's no evidence that existing vaccines & treatments don't work. We need to use them!
15/
A more infectious variant is very concerning, particularly when so much of the world remains unvaccinated.
But should we panic (as the markets did yesterday)? NO
There's no evidence that existing vaccines & treatments don't work. We need to use them!
15/
What can we do about Omicron?
-begin comprehensively testing air travelers (detect asymptomatic spread)
-implement a vaccine mandate for all domestic & international air travel to the US
-continue making vaccines available to the the world
16/16
-begin comprehensively testing air travelers (detect asymptomatic spread)
-implement a vaccine mandate for all domestic & international air travel to the US
-continue making vaccines available to the the world
16/16
• • •
Missing some Tweet in this thread? You can try to
force a refresh