Large study on boosters in Israel
Summary
>60 age
Risk of death among those who got infected: No difference between 2 or 3 dose groups
Risk of picking up an infection was 12 times lower after booster
Note: this was not a randomised trial
1/10
nejm.org/doi/full/10.10…
Summary
>60 age
Risk of death among those who got infected: No difference between 2 or 3 dose groups
Risk of picking up an infection was 12 times lower after booster
Note: this was not a randomised trial
1/10
nejm.org/doi/full/10.10…
The study compared the outcomes among 7,58,118 people who got booster with 85,090 who did not.
We do not know if there was a baseline difference in COVID- appropriate behaviour between the 2 groups.
Assuming no such difference, infection risk is reduced 12 fold by booster.
2/
We do not know if there was a baseline difference in COVID- appropriate behaviour between the 2 groups.
Assuming no such difference, infection risk is reduced 12 fold by booster.
2/
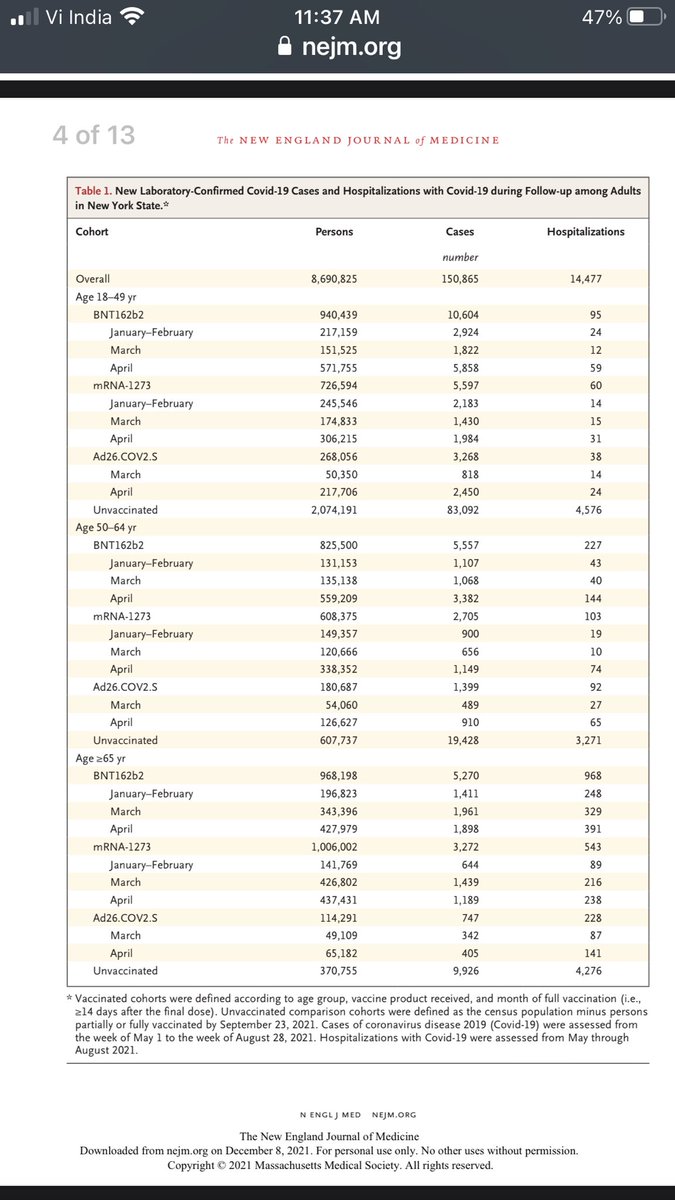
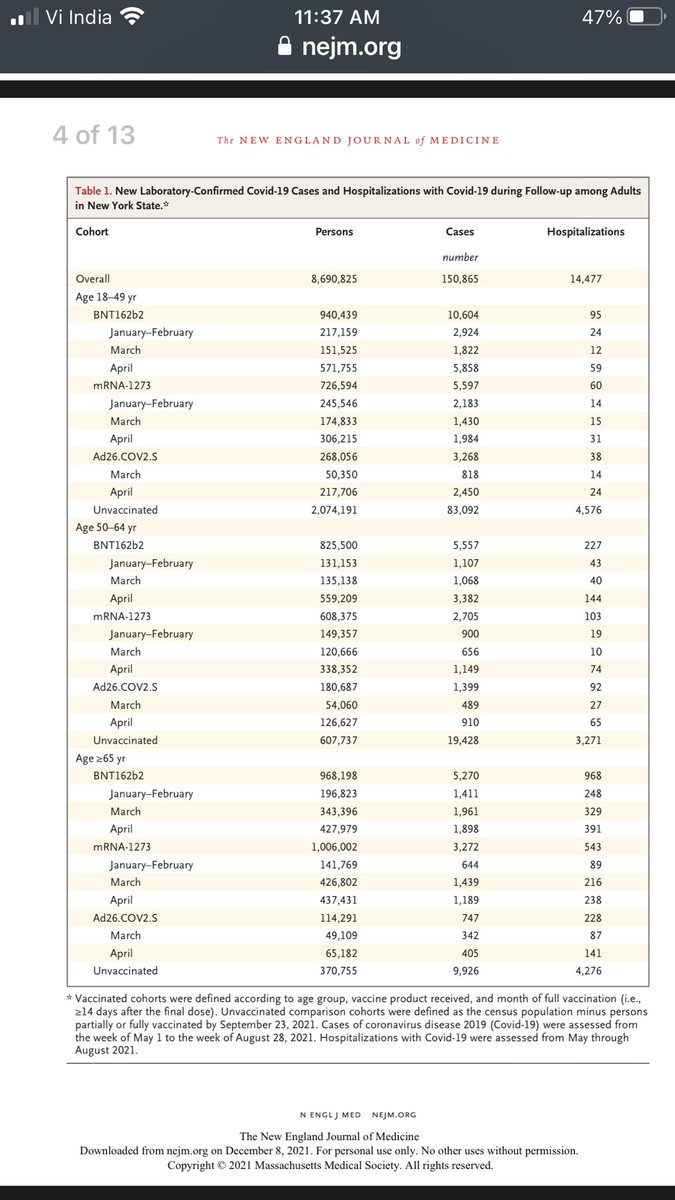
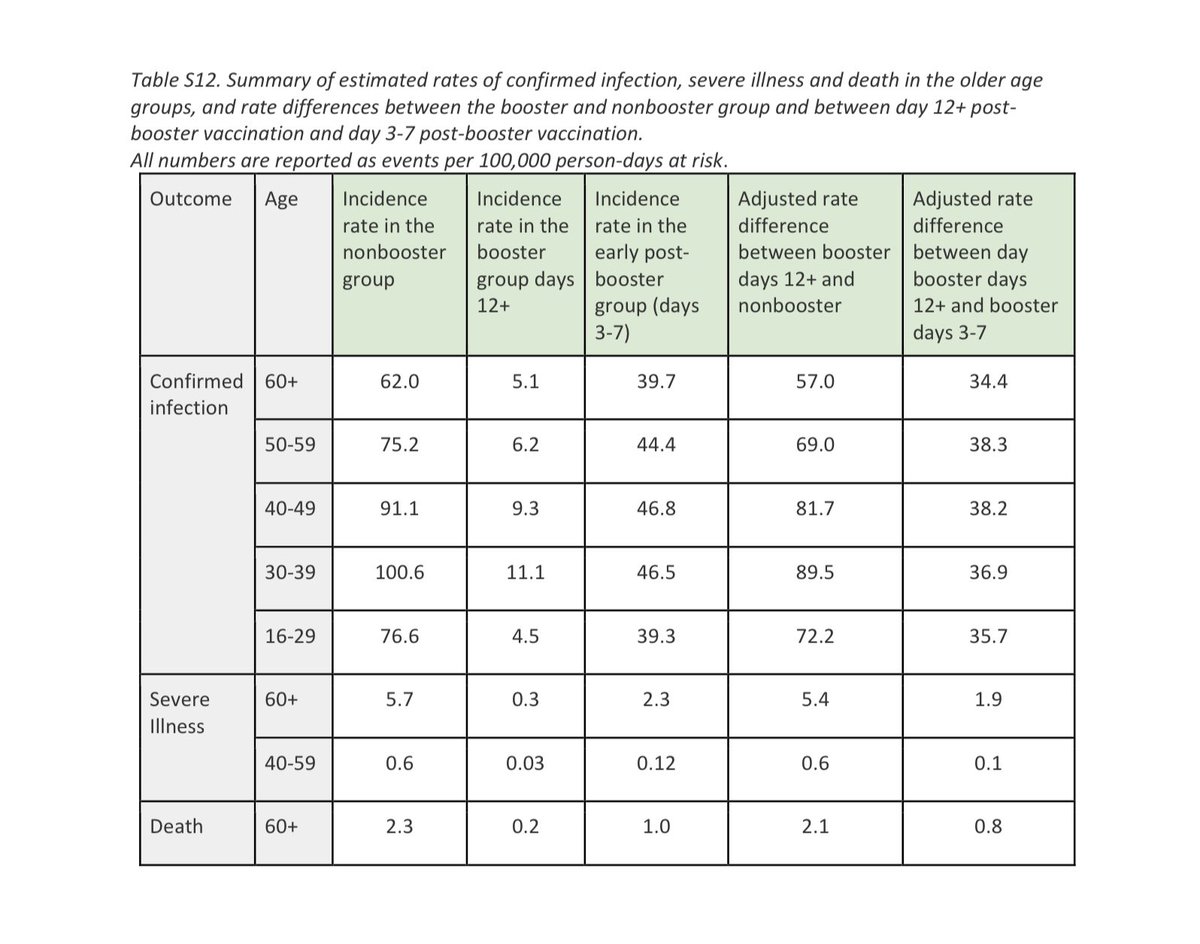
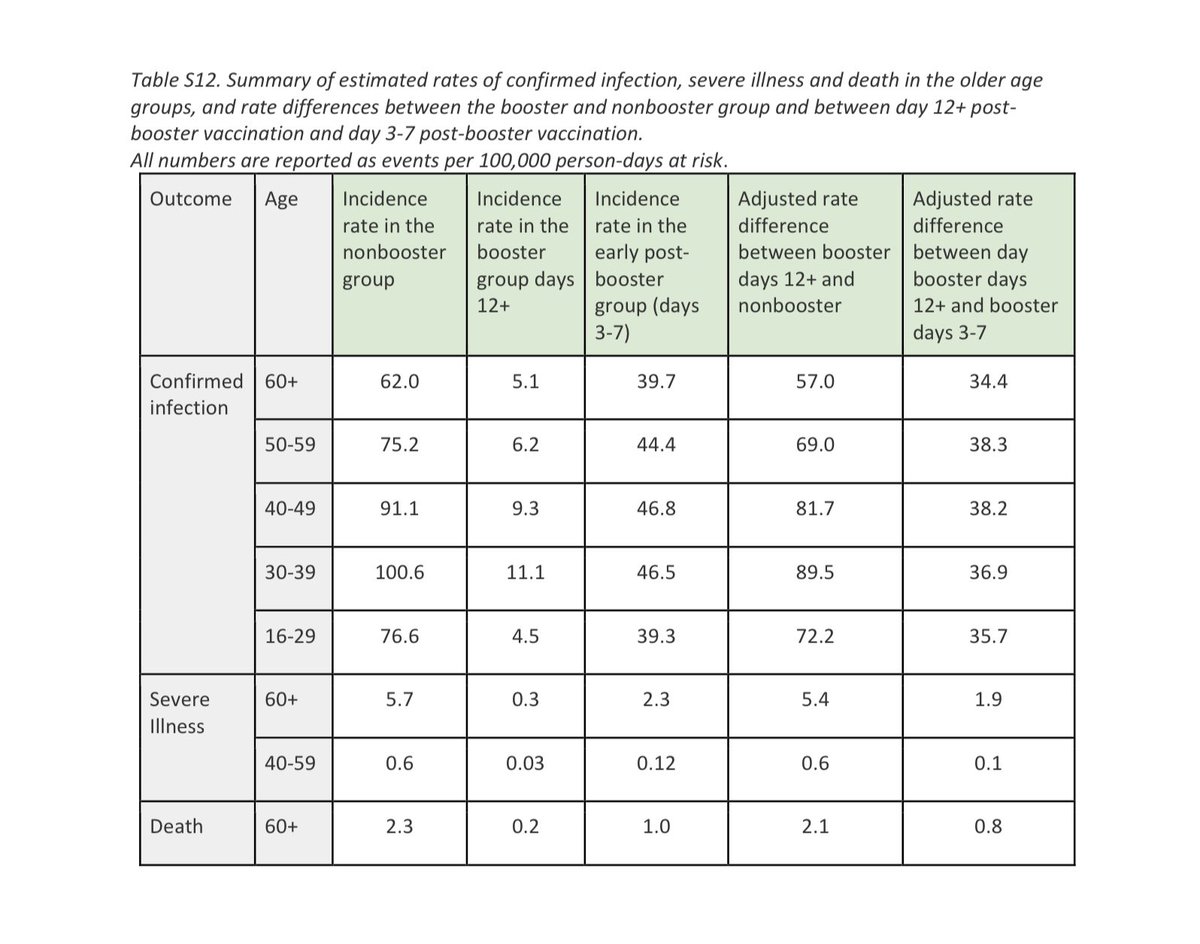
A few calculations based on the table:
Age > 60, non boosted (2 dose)
Infection rate 62 per 100,000 person days
Death rate 2.3
Ratio = 1 : 27
Age >60 (boosted)
Infection rate 5.1 per 100,000 person days
Death rate 0.2
Ratio = 1 : 26
(Ratio = chance of death if infected)
3/
Age > 60, non boosted (2 dose)
Infection rate 62 per 100,000 person days
Death rate 2.3
Ratio = 1 : 27
Age >60 (boosted)
Infection rate 5.1 per 100,000 person days
Death rate 0.2
Ratio = 1 : 26
(Ratio = chance of death if infected)
3/
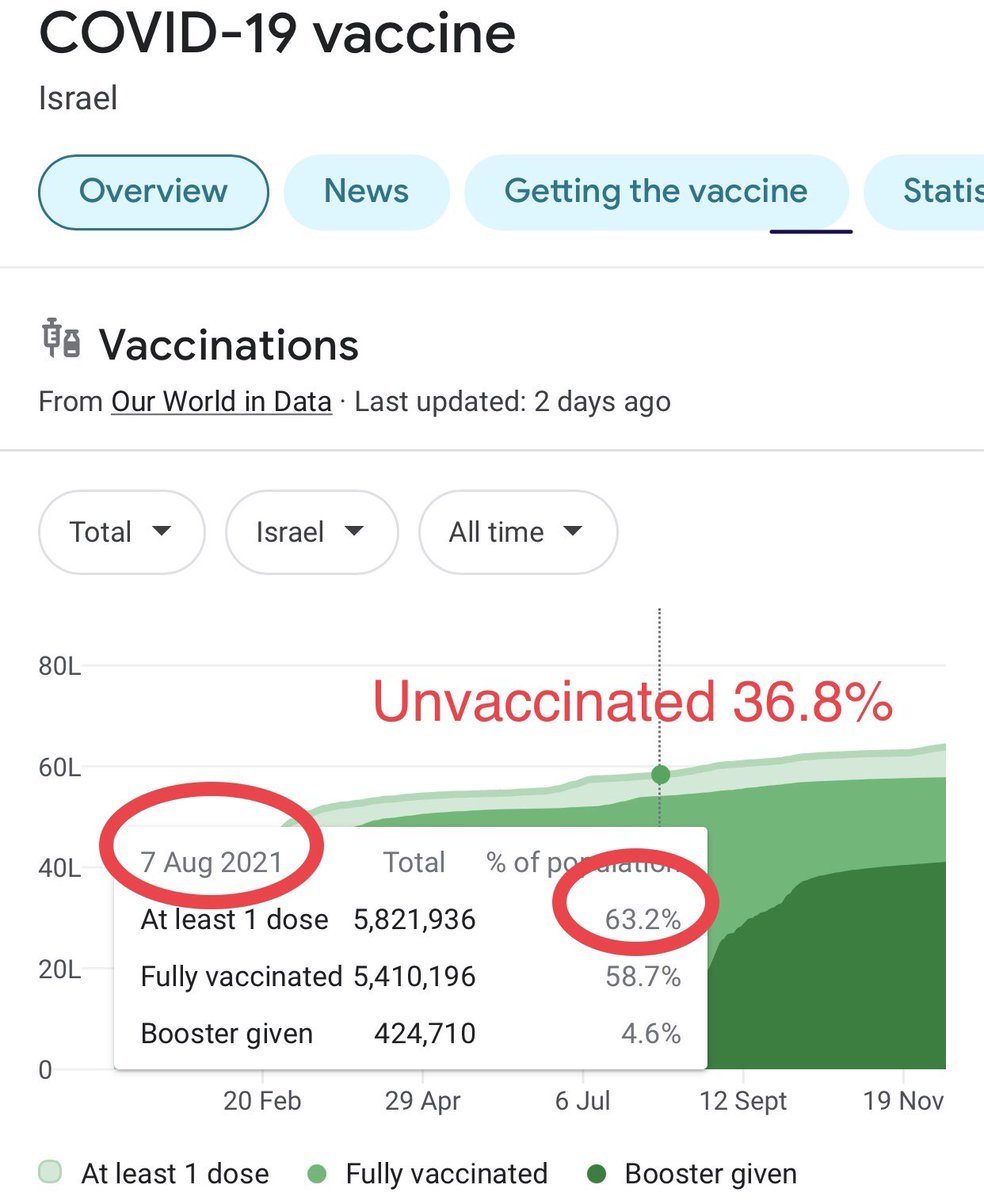
Unfortunately they did not report on unvaccinated people for comparison. At the beginning of the study (Aug 6) about 37% of the population was unvaccinated.
This could have served as a control group to see how the 2-dose group was actually doing. (Should not be difficult)
4/
This could have served as a control group to see how the 2-dose group was actually doing. (Should not be difficult)
4/
Observations from non-randomised studies are subject to multiple forms of bias which include differences baseline differences in Covid appropriate behaviour, testing threshold and demography, not all of which can be statistically corrected for.
5/
5/
The study was conducted during the most recent COVID surge in Israel, the starting date being August 6 and ending date September 29. 59% of the population had been fully vaccinated at the beginning of the study. 37% had been and vaccinated, but not included in the study.
6/
6/
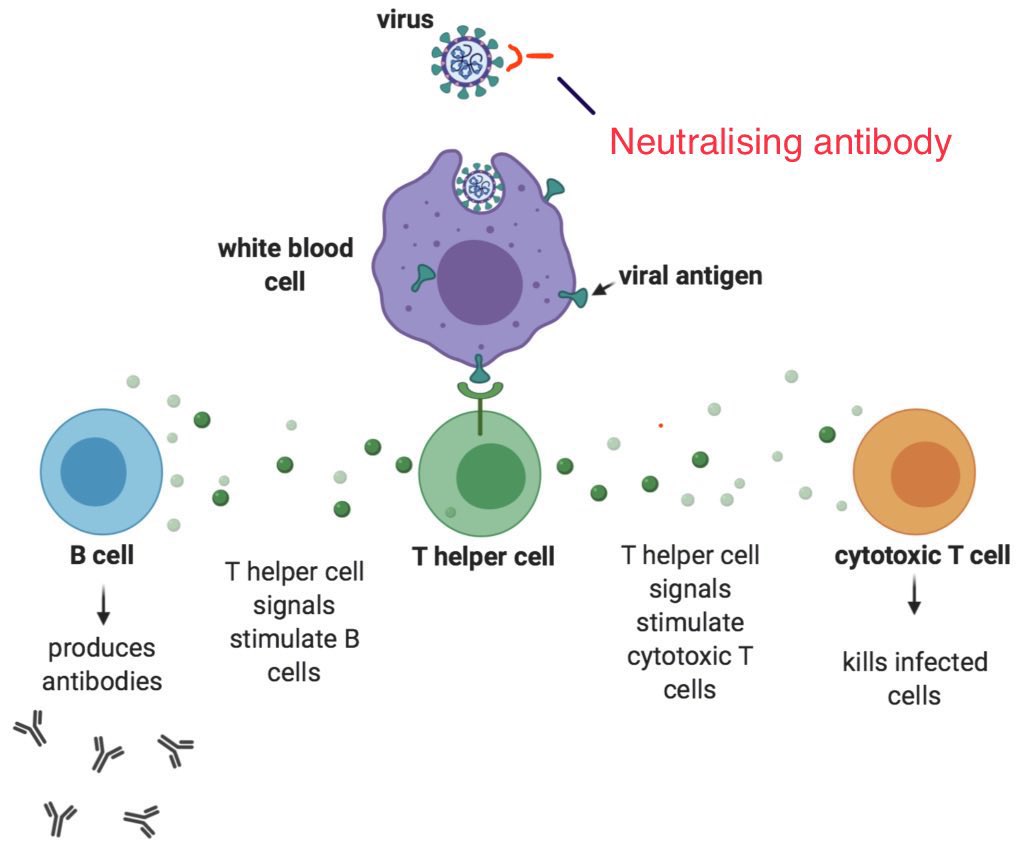
Apparently, the 3rd dose does not make the person ANY LESS LIKELY TO DIE in the event of an infection
This suggests that in the two-tiered immunity (1. infection 2. organ damage), the 2nd tier is “already maxed out” after 2nd dose, while the 1st tier (NAb) can be ‘topped up’
7/
This suggests that in the two-tiered immunity (1. infection 2. organ damage), the 2nd tier is “already maxed out” after 2nd dose, while the 1st tier (NAb) can be ‘topped up’
7/
What can be inferred from the study therefore is that a booster dose will provide a new window of protection from picking up infections.
What the body’s immune system does AFTER the infection sets in, appears to be already decided by the initial 2 dose series of vaccine.
8/
What the body’s immune system does AFTER the infection sets in, appears to be already decided by the initial 2 dose series of vaccine.
8/
What the booster dose apparently does, is to reduce the odds of picking up an infection (assuming no difference in CAB between groups) and its expected natural outcomes.
Fewer infections = fewer deaths.
9/
Fewer infections = fewer deaths.
9/
It will be appropriate to add that non pharma interventions are also effective at reducing infections.
Adherence to these will effectively reduce not only the total number of infections, but also the number of severe outcomes.
10/10
Adherence to these will effectively reduce not only the total number of infections, but also the number of severe outcomes.
10/10
• • •
Missing some Tweet in this thread? You can try to
force a refresh