“Immortal Time Bias” produces exaggerated positive results in observational studies. Thanks @DrToddLee for pointing it out
e.g. Booster studies give reliable results when subjects are randomised to booster or placebo. RCT ensures ~equal comparison.
1/9
academic.oup.com/aje/article/16…
e.g. Booster studies give reliable results when subjects are randomised to booster or placebo. RCT ensures ~equal comparison.
1/9
academic.oup.com/aje/article/16…
What is immortal time bias?
When a group under observation has a fixed advantage at the outset.
In heart transplantation VS non heart transplantation studies, this bias was first described (those who got the transplant had the opportunity to survive till they got operated)
2/
When a group under observation has a fixed advantage at the outset.
In heart transplantation VS non heart transplantation studies, this bias was first described (those who got the transplant had the opportunity to survive till they got operated)
2/
That is, the transplanted group were the healthier of the lot, they survived longer than those who died while waiting for surgery.
This was projected as an apparent outcome of transplant in some studies.
3/
This was projected as an apparent outcome of transplant in some studies.
3/
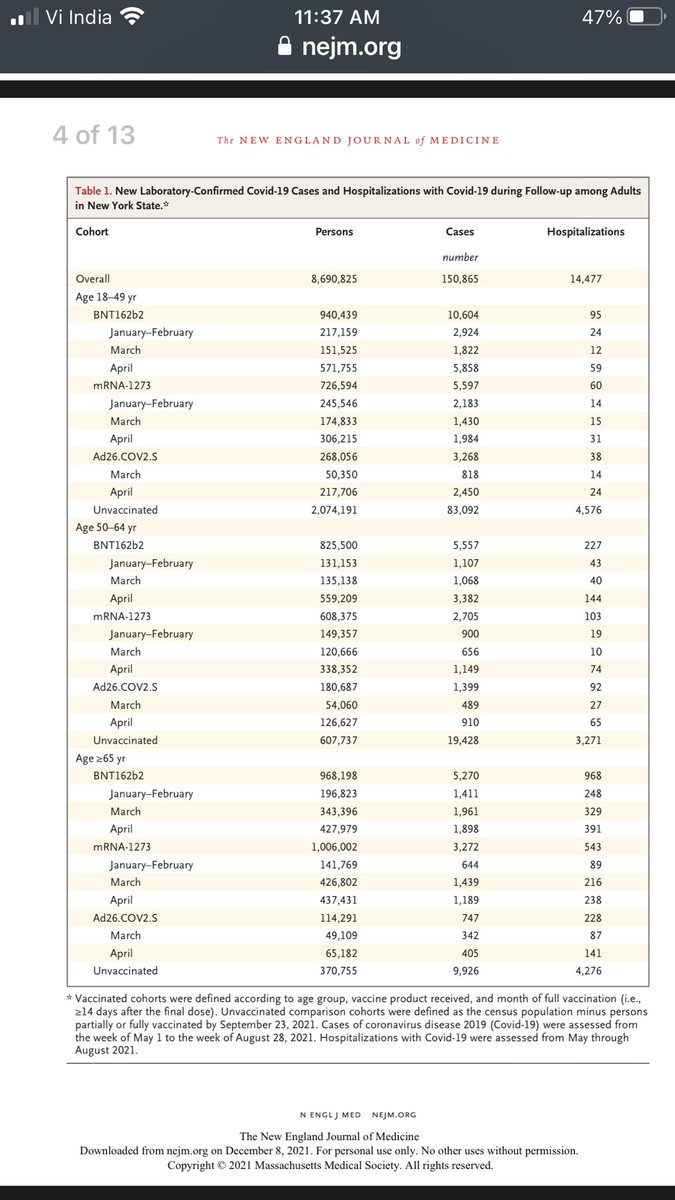
In the booster context, a non randomised observational study is prone to numerous bias, almost all of which favour the booster group.
The study was done during a surge of cases in Israel. Those who got the booster eventually had to meet one basic condition: “not to die”
4/
The study was done during a surge of cases in Israel. Those who got the booster eventually had to meet one basic condition: “not to die”
4/
Yes, though it sounds darkly funny, this is a form of bias. That is, only if you survived the pre-booster period will you be able to get the booster.
In other words, some people got “selected out” before being boosted simply because they died during the surge, or got ill.
5/
In other words, some people got “selected out” before being boosted simply because they died during the surge, or got ill.
5/
Such individuals remained in the two dose group, their outcomes got counted with the 2 dose group.
Those who were healthier and survived the early part of the surge, went on to get a booster dose because they felt well enough (and were alive to receive it).
6/
Those who were healthier and survived the early part of the surge, went on to get a booster dose because they felt well enough (and were alive to receive it).
6/
How do we know this bias altered the results?
The authors allude to this by calling the “Healthy Vaccinee Bias”
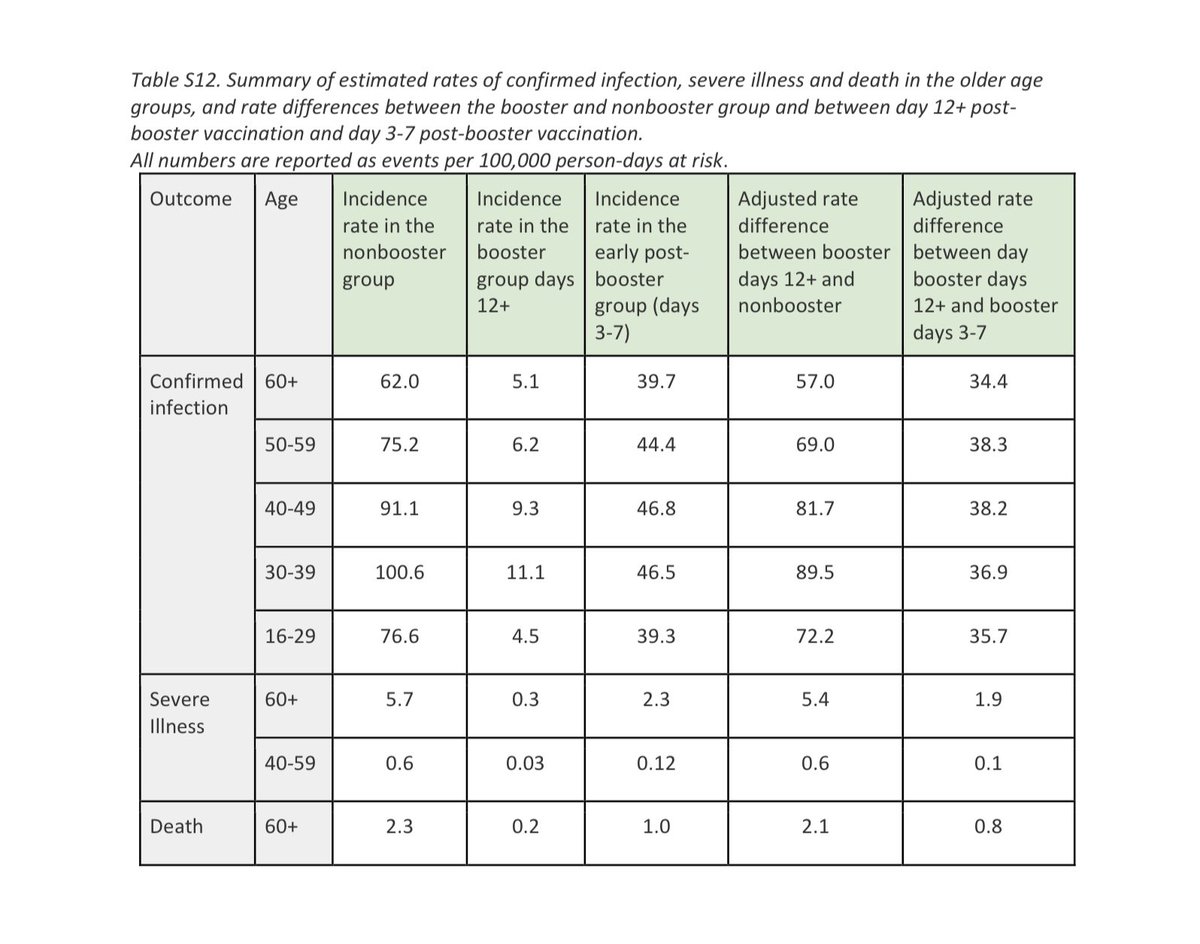
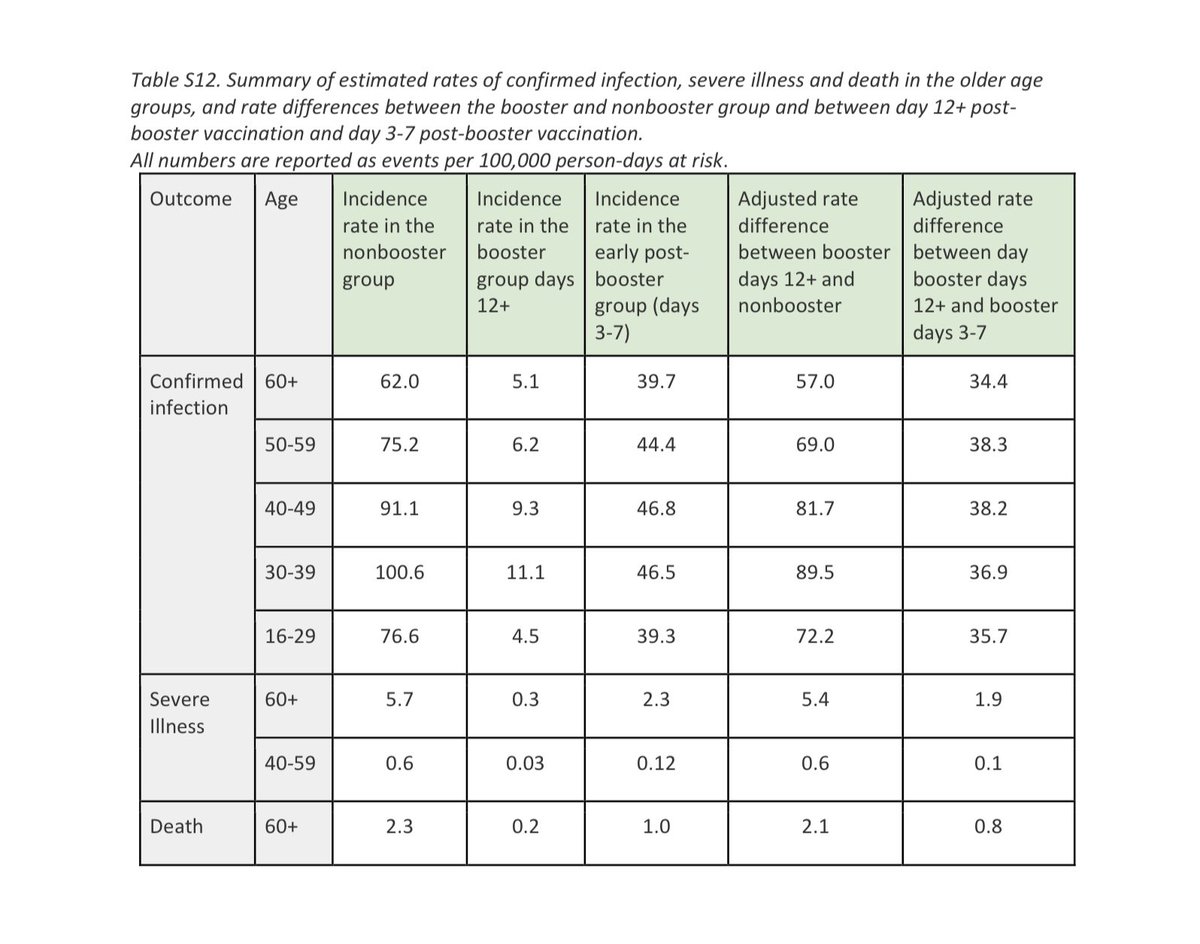
They do a secondary analysis, comparing the early 3-7 day period to post 2 weeks after booster.
And the difference is clear.
7/
The authors allude to this by calling the “Healthy Vaccinee Bias”
They do a secondary analysis, comparing the early 3-7 day period to post 2 weeks after booster.
And the difference is clear.
7/
This secondary analysis results in a dramatic drop in their original benefit estimate.
This is because the “immortal time bias” & “lower testing rate” bias are somewhat corrected for.
However, this does not correct for basic differences like covid appropriate behaviour.
8/
This is because the “immortal time bias” & “lower testing rate” bias are somewhat corrected for.
However, this does not correct for basic differences like covid appropriate behaviour.
8/
In summary, unless it is a randomised controlled trial, many forms of bias will creep in, and distort the conclusions in favour of the intervention.
This form of bias has been called out in several pharma studies.
9/9
This form of bias has been called out in several pharma studies.
9/9
• • •
Missing some Tweet in this thread? You can try to
force a refresh