An amazing study led by @emcat1 carefully dissecting the properties of omicron relative to other variants. TL;DR:
omicron shows:
-high levels of escape from vaccines with immunity partly restored post-3rd dose
-lower syncytia formation
-different preferred mechanism of cell entry
omicron shows:
-high levels of escape from vaccines with immunity partly restored post-3rd dose
-lower syncytia formation
-different preferred mechanism of cell entry
https://twitter.com/CVRinfo/status/1476580105426194432
First, the study predictably showed large reductions in neutralising antibodies for omicron compared to the original variant for all vaccines, with absolute levels lowest for AZ, and higher for both mRNA vaccines (highest for Moderna, and then Pfizer) 
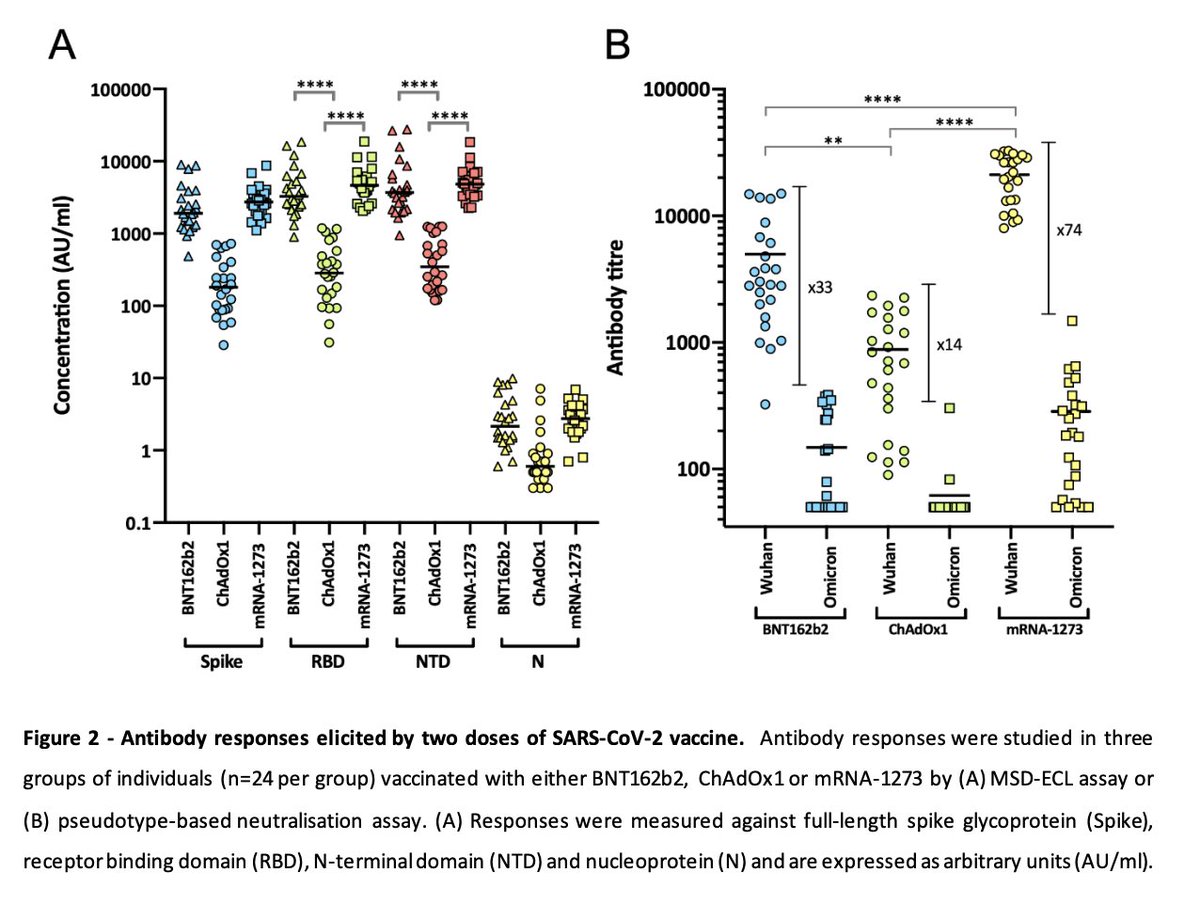
Boosting increased neutralising antibody titres, esp for those who had received 2 doses AZ, where this seems essential to partly restore immunity. Not sure what this means, but those with initial AZ boosted with mRNA had a higher proportion with measurable immunity (62% vs 25%).

But overall neutralising antibodies were still much lower with omicron compared to original wuhan strain even after boosting - starting at this lower level post-boosting means durability of protection may be lower.
So what does all this mean in terms of vaccine effectiveness?
So what does all this mean in terms of vaccine effectiveness?
Here, figure C shows vaccine effectiveness in the real-world, whereas figure D adjusts for duration since vaccination, so would show vaccine effectiveness ~2 wks after vaccination (so without waning). Overall, vaccine effectiveness much lower with omicron against becoming a case.
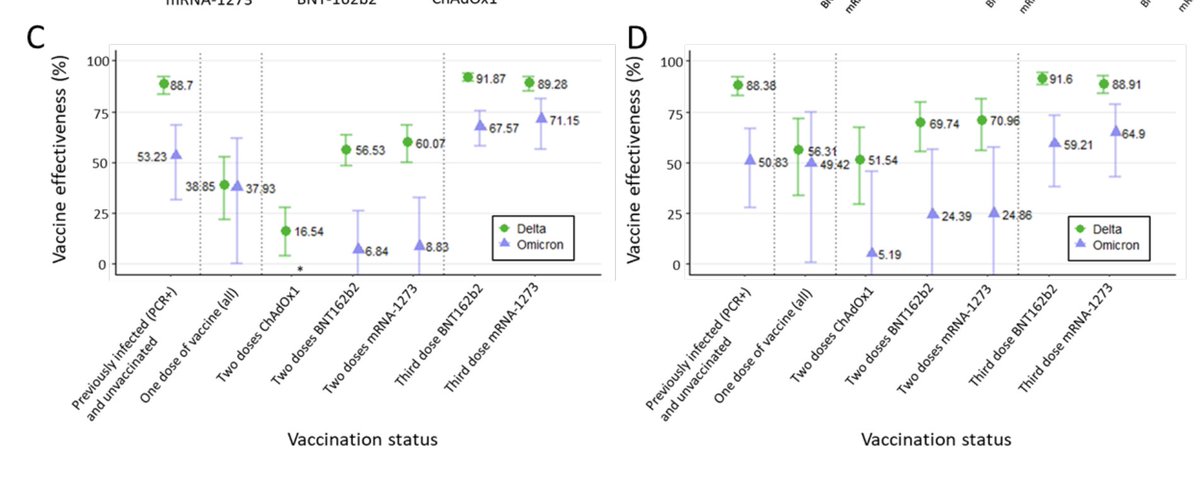
Effectiveness post-booster was similar to protection against the original variant post-2nd dose. So, the booster helped attain the same level of protection as 2 doses against the original variant. Previous infection provided higher protection than 2 doses but less than 3 doses.
All of this is vaccine effectiveness against becoming a confirmed case. Vaccine effectiveness against severe disease is much higher, as the Imperial study showed and likely to be more durable than effectiveness against preventing infections.
Because protection against infection is lower, including for those vaccinated/boosted compared to delta, even if protection against severe disease is unchanged with omicron compared to delta, overall risk may still be higher among vulnerable groups due to higher infection risk.
What about pathogenicity?
One of the indicators of pathogenicity of a virus is syncytia formation (fusion of cells with each other). This was a key feature of delta, potentially related to its higher severity. In the study, omicron did not produce syncytia - but delta did.
One of the indicators of pathogenicity of a virus is syncytia formation (fusion of cells with each other). This was a key feature of delta, potentially related to its higher severity. In the study, omicron did not produce syncytia - but delta did.
This may suggest lower pathogenicity compared with delta. While this correlates with many epidemiological studies, it's worth noting that only a few studies attempted to tease out *intrinsic severity* from reduced severity due to disproportionate infection of immune groups.
The PHS study and the recent Ontario study did not account for re-infections, & underascertainment of re-infections in the way the Imperial study did.
The Imperial study showed *intrinsic severity* was lower (but not by a lot). This correlates with findings from the study.
The Imperial study showed *intrinsic severity* was lower (but not by a lot). This correlates with findings from the study.
Replication of the virus in lung tissue was also lower than seen with delta and the Wuhan D614G virus (the one circulating in summer last year). Again might explain the lower *intrinsic severity* reported in the Imperial study.
Now to what I think is one of the most interesting insights in the paper. The preferred mechanism of entry into cells seems to have changed with omicron relative to previous variants.
There are two ways of entry into cells - delta preferentially employs fusion of the virus with the cell surface directly, while it seems omicron prefers a different mechanism to enter cells- it uses endosomes (a mechanism by which things outside the cell get taken into the cell)
What does this mean?
It's hard to know. Different mechanisms of entry may have different advantages in different tissues. So it may be less able to enter cells in the lung, for example, but more able to in other tissues.
It's hard to know. Different mechanisms of entry may have different advantages in different tissues. So it may be less able to enter cells in the lung, for example, but more able to in other tissues.
What this means for acute infection and long COVID will take time to figure out. But what's clear is that functionally and biologically omicron is very different to delta, and it's difficult to extrapolate what infection with omicron will mean - biologically.
It also highlights the huge potential for adaptation and flexibility of this virus. As the authors say:
"our work demonstrates that SARS-CoV-2 exhibits high antigenic and functional plasticity; further fundamental shifts in transmission and disease should be anticipated"
"our work demonstrates that SARS-CoV-2 exhibits high antigenic and functional plasticity; further fundamental shifts in transmission and disease should be anticipated"
It makes it very hard to predict how this virus will evolve, and what it will adapt towards. Vitally important to adopt the precautionary principle with omicron as we understand more, and adopt suppression strategies to reduce the probability of emergence of new variants.
Also, as the authors note:
" Even a variant that is less virulent with a very high transmission rate may still present a substantial risk to older people and those with co-morbidities, especially those with immunosuppression."
" Even a variant that is less virulent with a very high transmission rate may still present a substantial risk to older people and those with co-morbidities, especially those with immunosuppression."
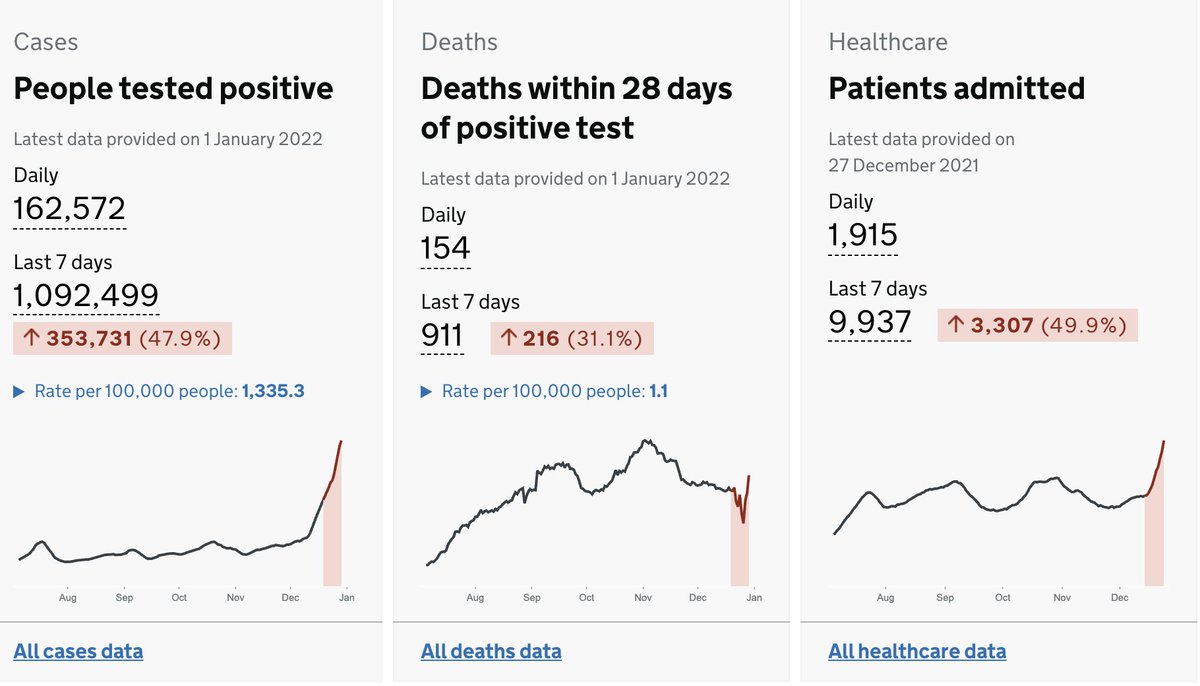
Given rapid spread of this variant, including in vaccinated people, and in those with prior immunity, public health measures are essential to prevent health services being overwhelmed, and limit spread to reduce the risk from long COVID, which is currently unknown with omicron.
Sorry, earlier tweet should've read:
"So, the booster helped attain the same level of protection as 2 doses against delta" rather than "against the original variant."
"So, the booster helped attain the same level of protection as 2 doses against delta" rather than "against the original variant."
• • •
Missing some Tweet in this thread? You can try to
force a refresh