
1/
Why does cold air make my kids' noses runny?
A weekend of playing in the snow made me wonder. I didn't do a deep dive but thought I'd share what I learned.
Why does cold air make my kids' noses runny?
A weekend of playing in the snow made me wonder. I didn't do a deep dive but thought I'd share what I learned.

2/
One of the earliest studies providing an explanation for cold-induced rhinorrhea came in 1985.
Subjects performed nasal breathing of cold/dry air (CDA) and warm/moist air.
🔑Only the CDA caused symptoms
🔑AND a rise in mast-cell mediators
t.ly/Y65a
One of the earliest studies providing an explanation for cold-induced rhinorrhea came in 1985.
Subjects performed nasal breathing of cold/dry air (CDA) and warm/moist air.
🔑Only the CDA caused symptoms
🔑AND a rise in mast-cell mediators
t.ly/Y65a

3/
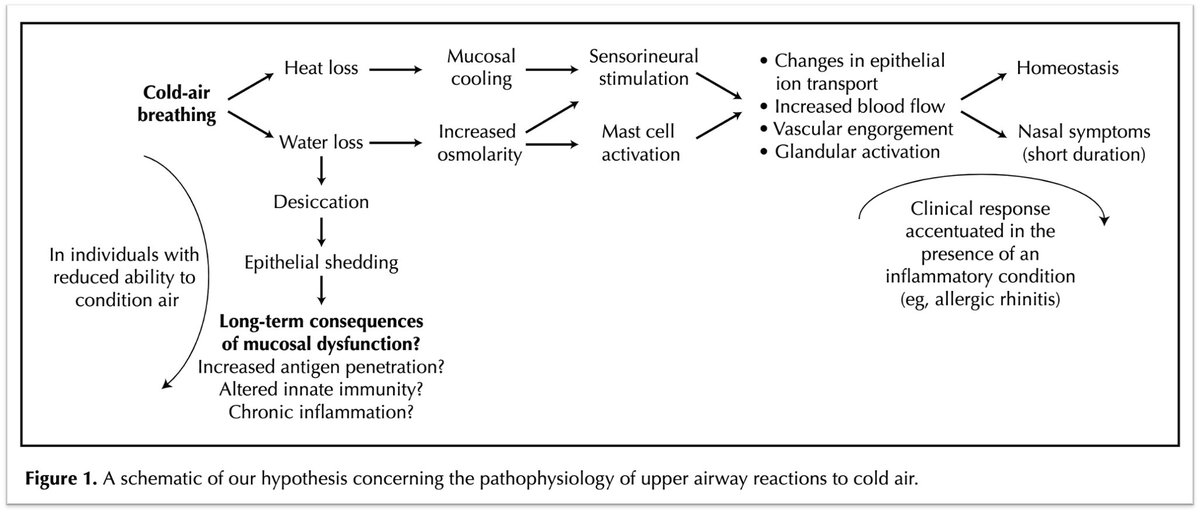
What's triggering the mast cell response? Is it the fact that the air is COLD or that it is DRY?
Unsurprisingly, both probably play a role.
🔑When DRY air meets the nasal mucosa, water evaporation leads to an increase in the osmolarity of the extracellular fluid.
What's triggering the mast cell response? Is it the fact that the air is COLD or that it is DRY?
Unsurprisingly, both probably play a role.
🔑When DRY air meets the nasal mucosa, water evaporation leads to an increase in the osmolarity of the extracellular fluid.
4/
Why does this matter? Hyperosmolarity is a known trigger of basophils and mast cells! This was demonstrated in a study published in 1981.
Exposure of basophils to hyperosmolar solutions (e.g., mannitol) led to the release of histamine.
t.ly/UVsF
Why does this matter? Hyperosmolarity is a known trigger of basophils and mast cells! This was demonstrated in a study published in 1981.
Exposure of basophils to hyperosmolar solutions (e.g., mannitol) led to the release of histamine.
t.ly/UVsF

5/
And histamine certainly plays a role in the symptoms of allergic rhinitis that mirror those in cold air mediated rhinitis (e.g., rhinorrhea).
t.ly/MFcX
And histamine certainly plays a role in the symptoms of allergic rhinitis that mirror those in cold air mediated rhinitis (e.g., rhinorrhea).
t.ly/MFcX
6/
But mast cells can't be the only mediator. This is suggested by experiments showing no decrease in cold air induced symptoms or histamine release by an antihistamine (azatadine).
Something else is going on.
t.ly/dK2u
But mast cells can't be the only mediator. This is suggested by experiments showing no decrease in cold air induced symptoms or histamine release by an antihistamine (azatadine).
Something else is going on.
t.ly/dK2u

7/
In addition to inducing basophil and mast cell mediator release, hyperosmolarity probably activates capsaicin-sensitive nociceptor nerves.
When hyperosmolar saline was applied via paper disk into a nostril, a runny nose resulted.
BUT...
t.ly/R7Pf
In addition to inducing basophil and mast cell mediator release, hyperosmolarity probably activates capsaicin-sensitive nociceptor nerves.
When hyperosmolar saline was applied via paper disk into a nostril, a runny nose resulted.
BUT...
t.ly/R7Pf

8/
...rhinorrhea was attenuated by lidocaine and capsaicin.
This suggests that hyperosmolarity stimulates sensory nerves.
...rhinorrhea was attenuated by lidocaine and capsaicin.
This suggests that hyperosmolarity stimulates sensory nerves.

9/
In fact, one study of skiers found that topical application of atropine blunted cold air-induced rhinorrhea supporting this being a cholinergic response.
t.ly/EFSO
In fact, one study of skiers found that topical application of atropine blunted cold air-induced rhinorrhea supporting this being a cholinergic response.
t.ly/EFSO
10/
Cooling of the nasal mucosa probably has some role as well. There are distinct cold-sensing receptors but whether they have a role in cold air-induced rhinorrhea isn't as clear.
t.ly/bhOf
Cooling of the nasal mucosa probably has some role as well. There are distinct cold-sensing receptors but whether they have a role in cold air-induced rhinorrhea isn't as clear.
t.ly/bhOf
11/
As for why some noses are runny in the cold...
The simplest explanation is that the secretions are aimed at restoring the homeostasis of the nasal mucosa after exposure the low-humidity dry air of the cold.
GREAT review: t.ly/DY8j
As for why some noses are runny in the cold...
The simplest explanation is that the secretions are aimed at restoring the homeostasis of the nasal mucosa after exposure the low-humidity dry air of the cold.
GREAT review: t.ly/DY8j
12/
Finally, there is an even simpler explanation that may be at play. When air is exhaled through the nose into a cold environment it rapidly cools. This leads to water vapor condensation.
And, a runny nose.
Finally, there is an even simpler explanation that may be at play. When air is exhaled through the nose into a cold environment it rapidly cools. This leads to water vapor condensation.
And, a runny nose.
• • •
Missing some Tweet in this thread? You can try to
force a refresh











