
1/ Yes! @NutritionMadeS3 -- please stay with this, it's important.
This goes back to what we were talking about last summer and why I keep drawing the distinction...
In fact, if you (and everyone else reading) would care to indulge me -- I'll unpack further...
This goes back to what we were talking about last summer and why I keep drawing the distinction...
In fact, if you (and everyone else reading) would care to indulge me -- I'll unpack further...
https://twitter.com/NutritionMadeS3/status/1501053917743960068
2/ Let's definitely grant for a moment that ApoB containing lipoproteins (which we'll call ApoB-Lp) are participants in the process of ASCVD.
Can we likewise consider there are disease states (whether genetic or acquired) that result in both changes in serum ApoB-Lp *and* ASCVD?
Can we likewise consider there are disease states (whether genetic or acquired) that result in both changes in serum ApoB-Lp *and* ASCVD?
3/ Monogenetic FH is certainly one I'd Put on the table.
In particular, a likewise constituent participant in the process of ASCVD are macrophages. Macrophages are nucleated immune cells and can thus suffer the same dysfunctional lipid metabolism we see with hepatocytes of MoFH.
In particular, a likewise constituent participant in the process of ASCVD are macrophages. Macrophages are nucleated immune cells and can thus suffer the same dysfunctional lipid metabolism we see with hepatocytes of MoFH.
4/ Please take a moment to read this study, @NutritionMadeS3 -- pubmed.ncbi.nlm.nih.gov/27680891/
I promise you'll find it quite interesting in this very context.
I promise you'll find it quite interesting in this very context.
5/ Naturally, this begs the very important question with regard to higher ApoB-Lp where *not* due to a dysfunction in lipid metabolism (obviously, this is why we're so interested in LMHRs).
But are there others who have increased ApoB/LDL without dysfunctional lipid metabolism?
But are there others who have increased ApoB/LDL without dysfunctional lipid metabolism?
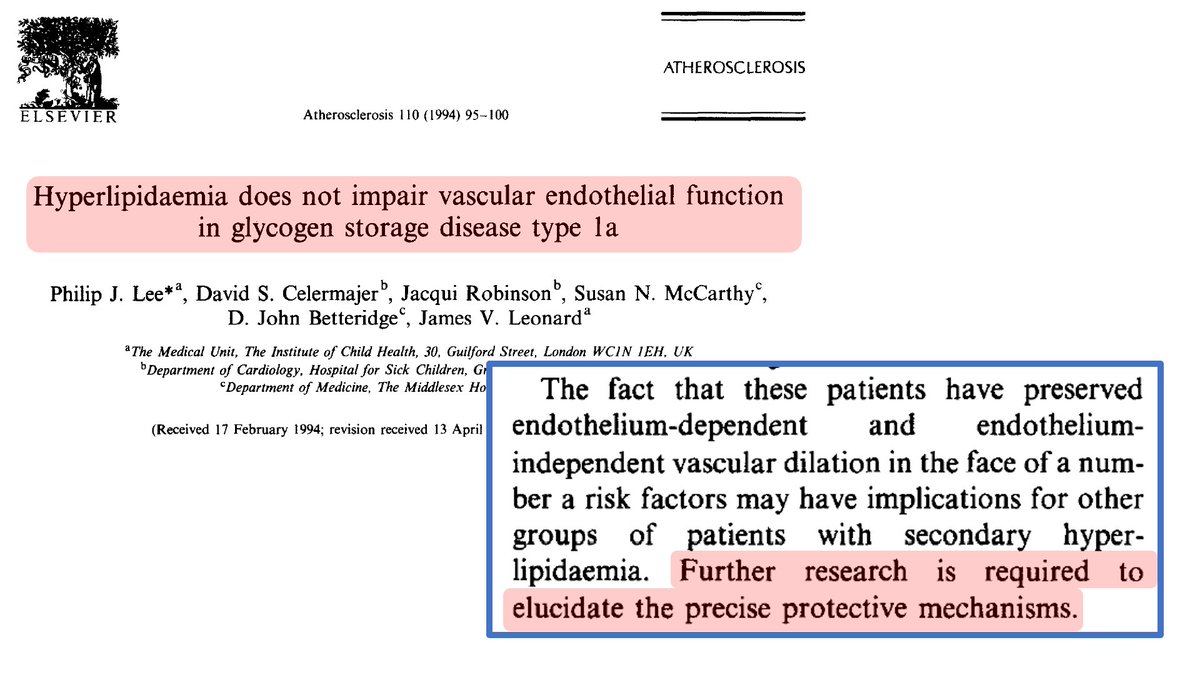
6/ Actually, there are a at least a couple dozen. But one that has had some decent study in particular is Glycogen Storage Disease (GSD). And we're especially interested in this disease given it somewhat simulates both fasting and keto (which deplete hepatic glycogen stores)...
7/ I went down a rabbit hole on GSD1a for a long time given it would have been a great analog to look at in this context. Do they have higher atherosclerosis? As it turns out -- not really... 
8/ This was another interesting one as well...

9/

10/ Anyway, I bring this up because I'm counting on you, @NutritionMadeS3 to remain curious about this. It's certainly possible the ApoB exposure (per lipid hypothesis) will simply be further confirmed through our research with LMHRs (and if so, we need to know soon!)...
11/ But if not -- if there's more to the story as we suspect, you're one of the people I'm counting on to be interested in following the data where it takes us. ;)
#science
#science
(study link: pubmed.ncbi.nlm.nih.gov/7857375/ )
(study link: pubmed.ncbi.nlm.nih.gov/20122579/)
(study link: pubmed.ncbi.nlm.nih.gov/12373574/)
• • •
Missing some Tweet in this thread? You can try to
force a refresh


