
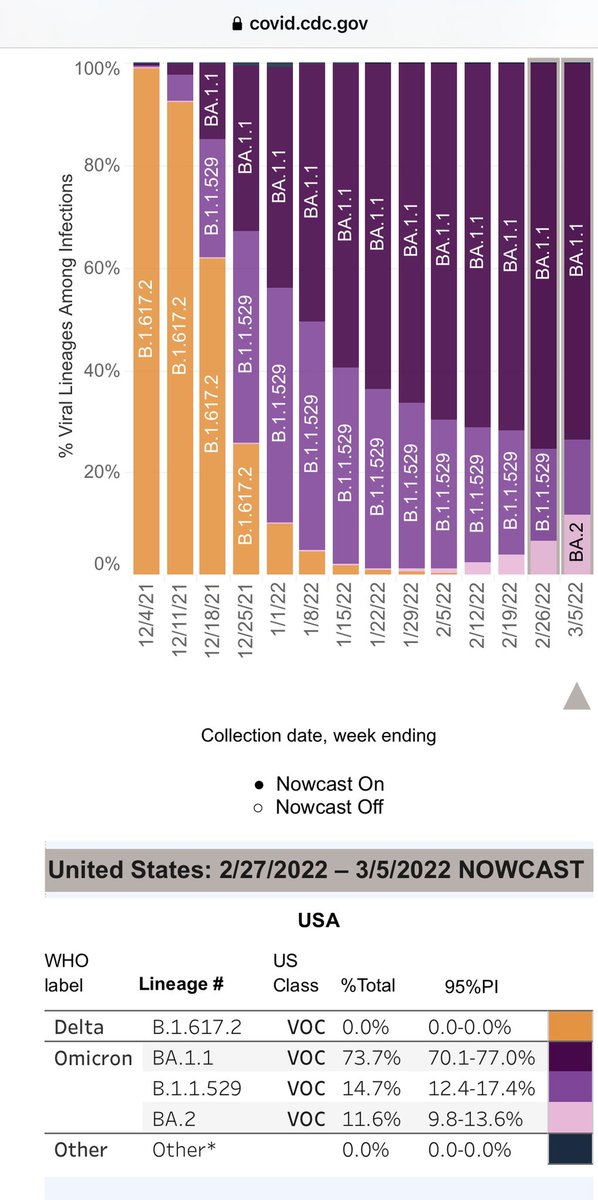
⚠️UPDATE—#BA2 is now 11.6% in US, up from 8.3% last week. It’s definitely increasing, as warned. #COVID19 still dropping, but BA2 is growing in underbelly—it’s a matter of when (not ‘if’) case drop plateaus, then reverses. Likely late April, early May.🧵
covid.cdc.gov/covid-data-tra…
covid.cdc.gov/covid-data-tra…

2) Where is #BA2 highest? In New England (HHS region 1), where BA2 is already 24% of all cases. It’s definitely outcompeting the old original #Omicron which is fading away.

3) #BA2 is not mild among unvaccinated and under-vaccinated populations. In Hong Kong 🇭🇰 where BA2 is very dominant, hospitals and morgues are overflowing. Hong Kong has never had a surge of this kind before - not until BA2 showed up.
https://twitter.com/DrEricDing/status/1498357688199176195
4) But some say HK hasn’t been hit hard by old Omicron, unlike US or UK. So what’s happening in England 🏴 then with its BA2 rise? Let’s check in— hospitalizations are rising in all age groups. Especially in kids 6-17, surging 26% in hospital admissions in one week. 👇
https://twitter.com/DrEricDing/status/1500983875207680006
5) Some are asking how bad is #BA2 in England 🏴 anyway— their last variant update was FEB 25th, but it shows roughly ~1/4th BA2– it’s not even that high of a percentage. Maybe it’s closer to half now but not dominant—yet hospitalizations up already.
assets.publishing.service.gov.uk/government/upl…
assets.publishing.service.gov.uk/government/upl…

6) How fast is the relative rise of #BA2 versus the emergence of other variants? Early on, it matched the old #Omicron for a while… slower now but still faster than older variants. This is not a good sign.

7) HOW IT STARTED… HOW ITS GOING… by region in the US, compare one month ago on Feb 5th… versus now March 5th data see anything wrong with the pink pie charts? #BA2 is growing. I’ve seen this rodeo 4 times before. New variants displace old ones for a reason—it’s not good sign.


8) Back to Hong Kong— just how bad is #COVID19 deaths in 🇭🇰 right now? It is almost “Holy Mary” bad. It’s higher than any record high that US or Europe has ever seen. When hospitals 🏥 & morgues overloaded, it’s not merely “with COVID”—it’s directly COVID. HK is undervaccinated.

9) If we just look at the recent (old) Omicron wave, HK’s surge makes the recent really bad Omicron wave look tepid (it’s not —it’s the second worst wave the US had). The new HK BA2 is that severe. Maybe the Us might fare better initially—but I worry about waning immunity by May.


10) Meanwhile, The good news is that #Omicron responds to Boosters well — 90-95% protection against hospitalization. However, 2 shots “basic” vax isn’t enough anymore versus Omicron—protection now only 70-79% depending on agent group. ➡️Note—70% is 3x worse than 90% if inverted.
https://twitter.com/DrEricDing/status/1500643406380425220
11) the secondary ATTACK RATES (infection in secondary household members and in workplaces) is also much higher with #Ba2 than other variants. 14.3% is quite high and about ~25% ⬆️ higher than BA1’s 11.4%. Basically it’ll cross infect more people. This is why it’s a bad sign.

12) Furthermore, in non-household settings, the secondary ATTACK RATE (cross infection to others) is 6.1% for #BA2. but that is 32.6% ⬆️ higher than BA1 (old Omicron). This again is not good.

13) REMINDER that #covidisairborne. Please try to mask - but if you don’t, please buy a HEPA filter or build a Corsi-Rosenthal Box 📦 filter. See thread 🧵 below 👇
https://twitter.com/drericding/status/1471054758085632002
14) #Ba2 is now ~1/4th of all cases in Ontario—even with incomplete sequencing data. This is a spike of 40% increase from last week alone.
https://twitter.com/dgbassani/status/1501261878076579840
15) Again, don’t be misled by falling cases. While total cases may be dropping (of the older variants), there can be an “under growth” in the underbelly, that when it becomes dominant, will crisscross and then cause a new surge. We have seen this before countless times.
https://twitter.com/GosiaGasperoPhD/status/1501067495469314051
16) Too many people are selfish and lacking in compassion during the pandemic. This is one of the fundamental reasons that #CovidIsNotOver. I explore many of the fallacies below 👇
https://twitter.com/drericding/status/1500638716460740609
17) The trends for #BA2 in England 🏴 are quite alarming. 👇
https://twitter.com/DrEricDing/status/1501532919894061057
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















