The latest results from the #REACT study by @imperialcollege and @IpsosMORI are out, and whilst overall prevalence is lower, there's evidence that in the 55 and over age groups it is on an upward trend, consistent with a recent increase in admissions.
A summary 🧵
1/
A summary 🧵
1/

Overall prevalence is down from Round 17 (4.4%) to 2.9%, and within the Round (8th Feb to 1st Mar) R is estimated at 0.94, although as noted above for 55+ it is put at 1.04.
Although falling, it's still the 2nd highest ever level recorded by REACT by some margin.
2/
Although falling, it's still the 2nd highest ever level recorded by REACT by some margin.
2/

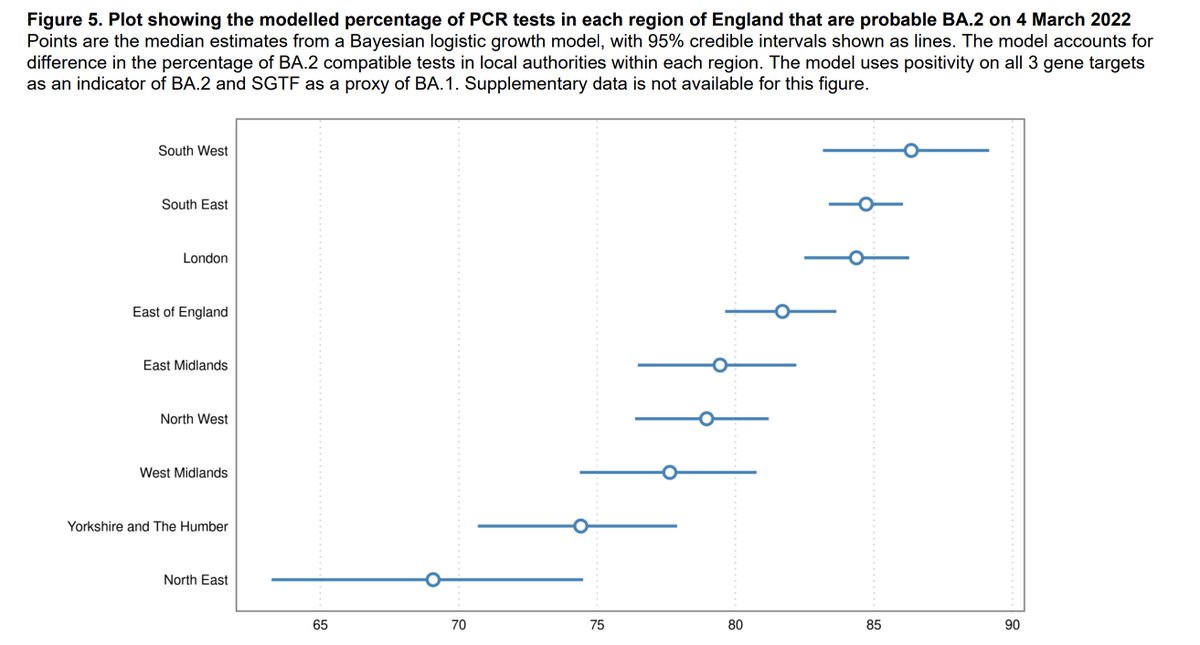
Regionally, most regions clearly fell from Round 17, but in contrast the South West and South East showed small, although not statistically significant increases, and along with London were the highest.
3/
3/

At lower tier LA level, 6 were in London, and the other four were clustered in what some in my locality will still (usually without much affection) remember as the old Avon area (Bristol, South Glos, BANES and North Somerset).
4/
4/

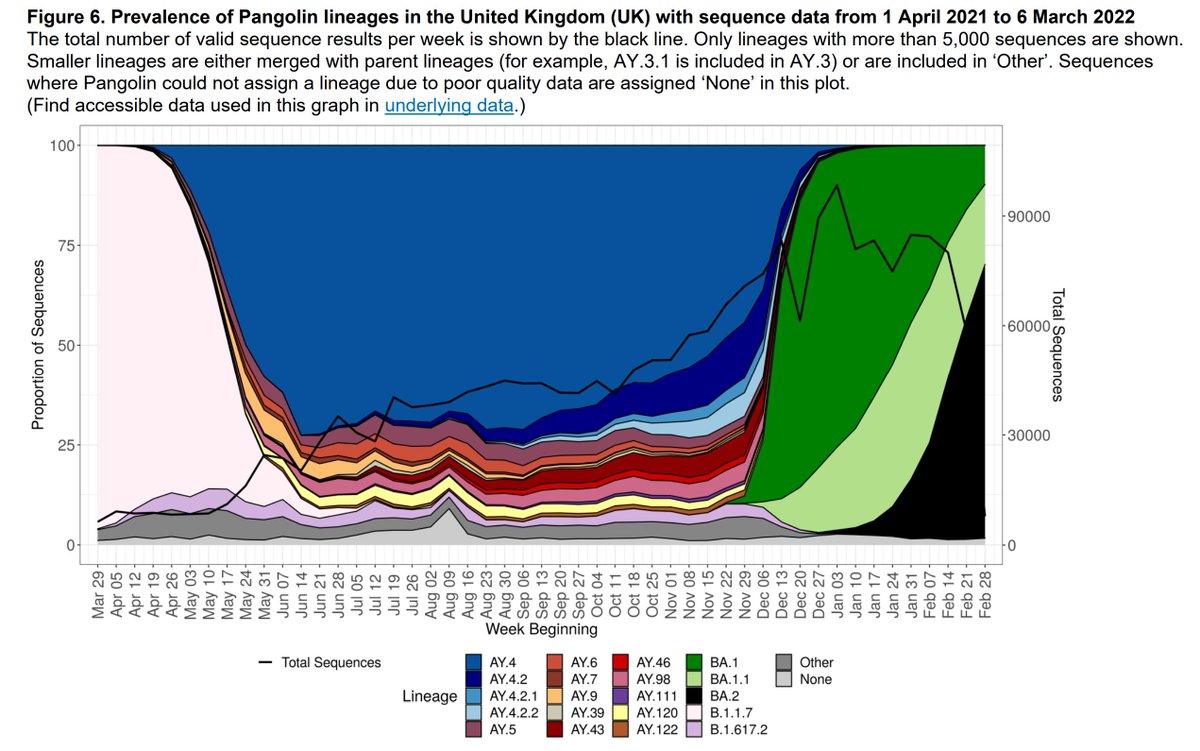
The proportions of BA.2 were highest in the SW and London too, and indeed the pattern here is very similar to the overall prevalence levels too, reflecting the growth advantage that BA.2 has, estimated at an additive rate of 0.4 to Rt.
5/
5/

Indeed, by the end of the round the proportion of BA.2 cases was approaching 50% of the total. And remember Delta? Over the whole round only 1 of the 1,195 cases sequenced was found to be that variant.
6/
6/

By age you can see here how the greatest falls from Round 17 are in the younger age bands. At older ages the falls are much lower and as noted earlier, within the Round there was evidence that over 55 prevalence was in fact increasing again.
7/
7/

A summary here of all the 18 rounds that this fantastic study has produced over the last two years. It's been a great source of data to complement other estimates of prevalence within England, and I'd like to thank all those involved over that period.
8/8
8/8

And here's the link to the report, with much more analysis than I've covered in my summary thread.
9/8
spiral.imperial.ac.uk/bitstream/1004…
9/8
spiral.imperial.ac.uk/bitstream/1004…
• • •
Missing some Tweet in this thread? You can try to
force a refresh