
I have been *waiting* for this type of extensive autopsy study to be be performed since I first learned about #COVID19. 3/2020-3/2021
N=44 autopsies; Brains = 11
Great care taken to be performed within 24 hrs of death.
None vaccinated. Prior to variants.
cc: @drjudymelinek 🧠
N=44 autopsies; Brains = 11
Great care taken to be performed within 24 hrs of death.
None vaccinated. Prior to variants.
cc: @drjudymelinek 🧠
https://twitter.com/fearnley_k/status/1532367164161810432

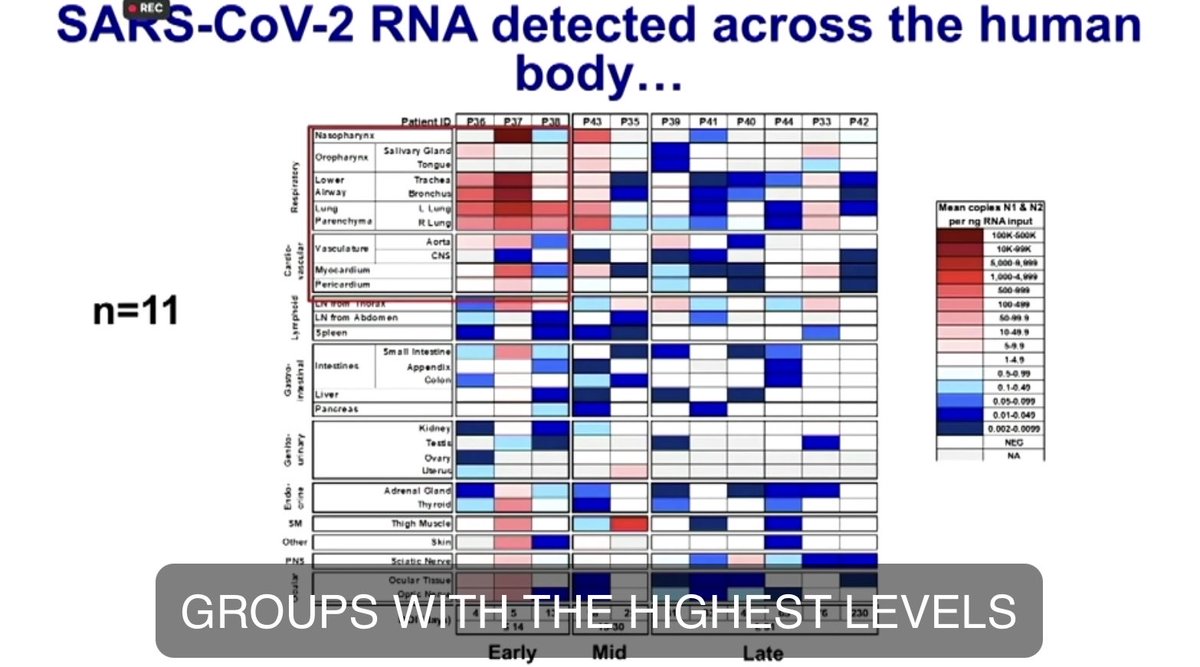
Alt text: figure shows viral RNA was detected in every brain structure/region they tested in deceased patients with #COVID19 (n=11)
Link to presentation: videocast.nih.gov/watch=45296?jw…
Link to presentation: videocast.nih.gov/watch=45296?jw…
They have full body data on these 11 patients including the brain.
Photo 1: SARSCOV2 RNA by PCR
Photo 2: subgenomic RNA overlaid on #SARSCOV2 sgRNA
Photo 3: Demographics
Photo 4: Clinical Summary
Photo 1: SARSCOV2 RNA by PCR
Photo 2: subgenomic RNA overlaid on #SARSCOV2 sgRNA
Photo 3: Demographics
Photo 4: Clinical Summary



4/ Should have started numbering…
Preserved more than 10k specimens for downstream analysis across 85 distinct anatomic sites and body fluids.
Fresh tissue and body fluids were preserved for downstream analysis in RNA later by droplet digital PCR assay for SARSCOV2 RNA
Preserved more than 10k specimens for downstream analysis across 85 distinct anatomic sites and body fluids.
Fresh tissue and body fluids were preserved for downstream analysis in RNA later by droplet digital PCR assay for SARSCOV2 RNA
5/ Assessed for qPCR for subgenomic RNA which is thought to be a marker of recent viral replication.
As well as high throughput single genome amplification and sequencing to compare diversity of #SARSCOV2 spike gene within and across anatomic compartments.
As well as high throughput single genome amplification and sequencing to compare diversity of #SARSCOV2 spike gene within and across anatomic compartments.
6/ Flash frozen tissue and fluids were collected for cell culture to evaluate for replication competent virus.
Research tissues were formalin fixed for histopathologic analysis as well as in situ hybridization (ISH) and immunohistochemistry (IHC) to query cellular tropism.
Research tissues were formalin fixed for histopathologic analysis as well as in situ hybridization (ISH) and immunohistochemistry (IHC) to query cellular tropism.

7/ Defined persistence as detection of all RNA in tissues > or = to 31 days post initial #COVID19 symptom onset. Detected subgenomic RNA in > 300 samples.
Then tested 50 samples from 20 patients in vero culture and successfully cultured virus from 25 anatomic locations in 9 pts
Then tested 50 samples from 20 patients in vero culture and successfully cultured virus from 25 anatomic locations in 9 pts

8/ In these tissues, a cytopathic effect and an increase in #SARSCOV2 subgenomic RNA levels in cell culture supernatant relative to levels in original tissue homogenant were observed confirming replication competent virus.
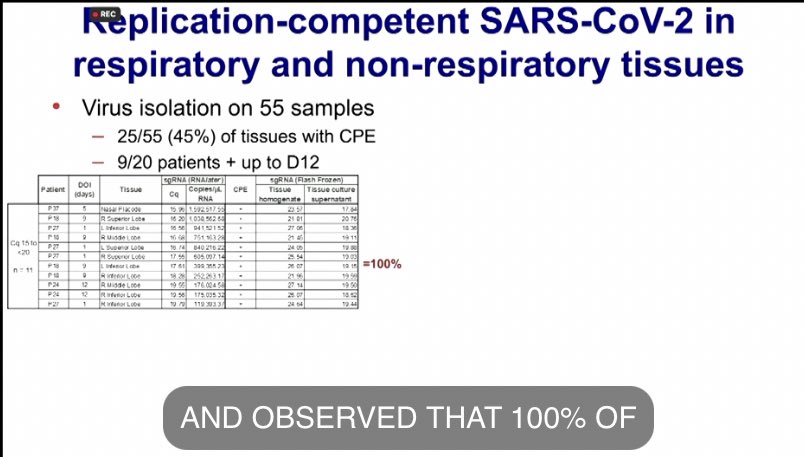
9/ 100% of tissues with a subgenomic RNA cycle threshold between 15 and 20 had replication competent virus.
This number decreased to 64.3% of tissues that had CT value between 20 and 25.
And further decreased to 31.1% of tissues that had a CT value between 25 and 30.
This number decreased to 64.3% of tissues that had CT value between 20 and 25.
And further decreased to 31.1% of tissues that had a CT value between 25 and 30.
10/ No replication of virus was detected in tissues with cycle threshold of 30 or higher.
Isolated replicating #SARSCOV2 from nasal placode, sinus turbinate, bronchus, lung, cornea & sclera of the EYE!, the jejunum, the mediastinal lymph node, the heart, and the adrenal gland.
Isolated replicating #SARSCOV2 from nasal placode, sinus turbinate, bronchus, lung, cornea & sclera of the EYE!, the jejunum, the mediastinal lymph node, the heart, and the adrenal gland.

11/ Robust framework showing that you can perform RNA and/or subgenomic RNA on tissue to determine if it likely to have replication competent virus without having to perform cell culture in a BSL3 setting (a limited resource)

12/ Using the ddPCR and sqRNA qPCR as a guide, we used ISH probing the SPIKE region of the SARSCOV2 genome to validate our PCR assays & to determine cell type specificity within tissues
Positive staining found in all tissue groups, small panel here that highlights ISH staining:
Positive staining found in all tissue groups, small panel here that highlights ISH staining:

13/ Displayed in first row, in order from left to right
a) Frontal Lobe
b) Corpus callosum (early case)
c) Cerebellum (late case)
d) Cervical spinal cord (late case)
a) Frontal Lobe
b) Corpus callosum (early case)
c) Cerebellum (late case)
d) Cervical spinal cord (late case)

14/ Second row:
e) Follicular cells of Thyroid
f) Stratified squamous epithelium of the esophagus + stroma of a capillary (#)
g) Mononuclear leukocytes within the white pulp of the spleen
h) Colonic epithelium (*) and mononuclear cells within the stroma of the appendix (#)
e) Follicular cells of Thyroid
f) Stratified squamous epithelium of the esophagus + stroma of a capillary (#)
g) Mononuclear leukocytes within the white pulp of the spleen
h) Colonic epithelium (*) and mononuclear cells within the stroma of the appendix (#)

15/ Third row:
i) Endocrine secretory cells of the adrenal gland
j) Stromal cells of the post menopausal ovary
k) Sertoli cells and maturing germ cells of the seminiferous tubule of the testes
l) Endometrial gland epithelium and stromal cells of a PREMENOPAUSAL UTERUS
i) Endocrine secretory cells of the adrenal gland
j) Stromal cells of the post menopausal ovary
k) Sertoli cells and maturing germ cells of the seminiferous tubule of the testes
l) Endometrial gland epithelium and stromal cells of a PREMENOPAUSAL UTERUS

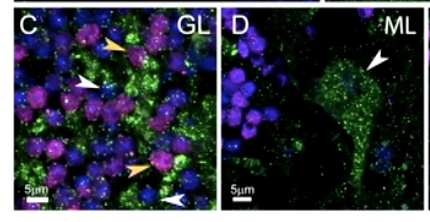
16/ Evaluated SARSCOV2 cellular tropism within the cerebellum & other regions of the brain via fluorescent IHC and confocal microscopy.
Blue = cerebellum cell nuclei
Green = #SARSCOV2 nucleocapsid
Neurons = magenta
ML = molecular layer
GL = granular layer
WM = white matter
Blue = cerebellum cell nuclei
Green = #SARSCOV2 nucleocapsid
Neurons = magenta
ML = molecular layer
GL = granular layer
WM = white matter

17/ A) Low magnification visualization of no antibody control
B) All specific protein expression (higher magnification of B shown in C, D, E shows specific cell type infection)
B) All specific protein expression (higher magnification of B shown in C, D, E shows specific cell type infection)

18/ C) Positive neurons indicated by yellow arrows, other unidentified cells indicated by white arrows are also associated with viral protein in the granular layer
D) Purkinje cells adjacent to the molecular layer are infected
D) Purkinje cells adjacent to the molecular layer are infected
19/ E) In rare instances, blood vessels adjacent to the granular layer and white matter were associated with viral protein

20/ This table summarizes the 36 cell types and hyaline membranes across the body and brain that were ISH positive for #SARSCOV2 SPIKE RNA in our cohort

21/ Final study aim was to determine if #SARSCOV2 evolves in different anatomical compartments within the same patient.
High throughput single genome sequencing to analyze SPIKE gene variant sequences from 46 tissues from 6 patients.
P18 = identical across all compartments
High throughput single genome sequencing to analyze SPIKE gene variant sequences from 46 tissues from 6 patients.
P18 = identical across all compartments

22/ P19 = Detected a single synonymous mutation (blue) in a minor variant in the right superior lung lobe
Overall, these 2 patients demonstrate that #SARSCOV2 can infect cells in non-respiratory tissues without requiring changes in the SPIKE genome.
Overall, these 2 patients demonstrate that #SARSCOV2 can infect cells in non-respiratory tissues without requiring changes in the SPIKE genome.

23/ P27 = synonymous mutations (blue) were detected both within the respiratory tract and outside of it, specifically in the mediastinal lymph node and the left and right ventricle of the heart.

24/ P33 = Unable to sequence many tissues as a late case, there were 2 distinct haplotypes detected within the thoracic lymph node

25/ They sequenced brain samples from 2 patients, which revealed non-synonymous mutations between haplotypes within the CNS and the rest of the body, specifically in the dura mater for P36 and the hypothalamus and thalamus in P38. #COVID19 #NeuroCOVID

26/ "These results indicate within the brain, that #SARSCOV2 is subject to the development of genetic compartmentalization...and exploring the mechanisms behind this will be...important... future...work..." (trails off somberly) #COVID19 #NeuroCOVID #LongCOVID

@threadreaderapp please unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh









