.@drpwh62 and I supervised soon-to-be Drs Angela Chen and Neha Ravi in a #LGBTQI+ literature review. Very impressed to see students present 'off podium' with minimal notes at the @BondUniversity MD conference! #MedEd 1/5 

The review looked at the gap between medical students and consultancy/attending practice. This is the career stage with the least research, and yet makes the biggest difference to eventual specialist workforce #LGBTQI representation. 2/5
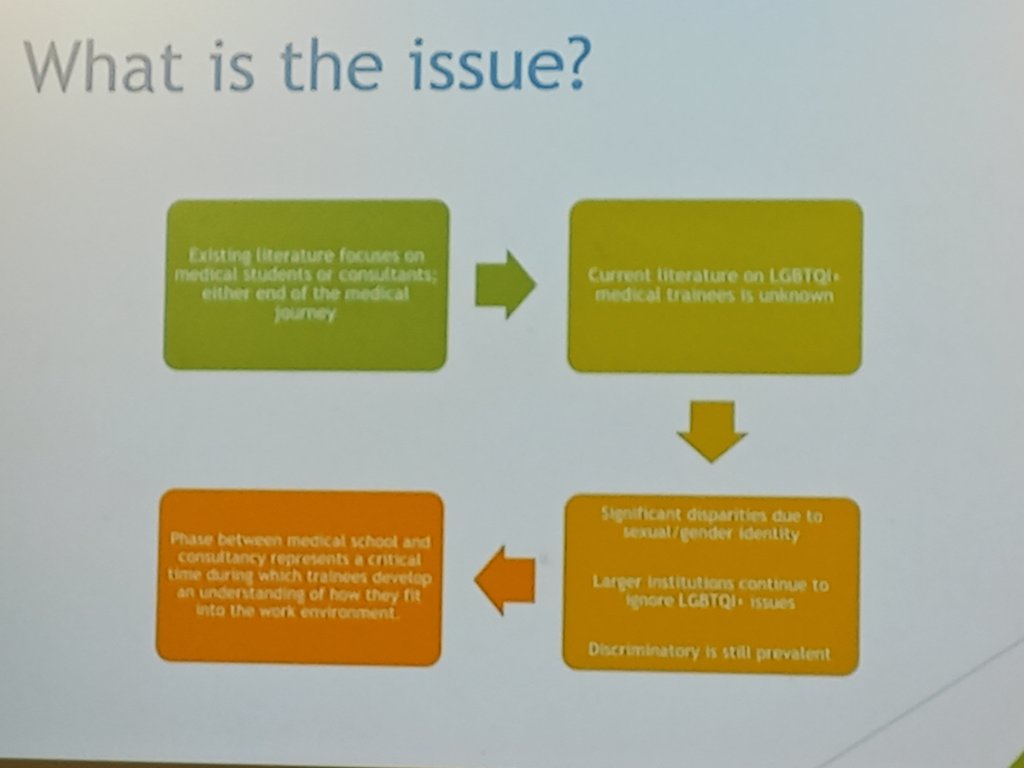
There were just 19 studies, and the results were as awful as expected. Bullying, discrimination, poor mental health, burnout, and lots of emotional labour. There were risks in both disclosing and not disclosing personal #LGBTQI identity. 3/5

Surveys have low response rates and can't untangle complexity, there's a lack of qualitative data, and for research about #DiversityandInclusion there was a distressing lack of recognition of diversity, with most studies lumping the whole #LGBTQI population together. 4/5

So- major research gaps identified for #LGBTQI pre-specialist doctors. These are opportunities for #DiversityandInclusion advocates/programmes, because medical students don't become consultants/attendings by magic. Let's get onto it! 5/5
• • •
Missing some Tweet in this thread? You can try to
force a refresh