NEXT Speaker : VA ecmo for which patients?
Alain COMBES
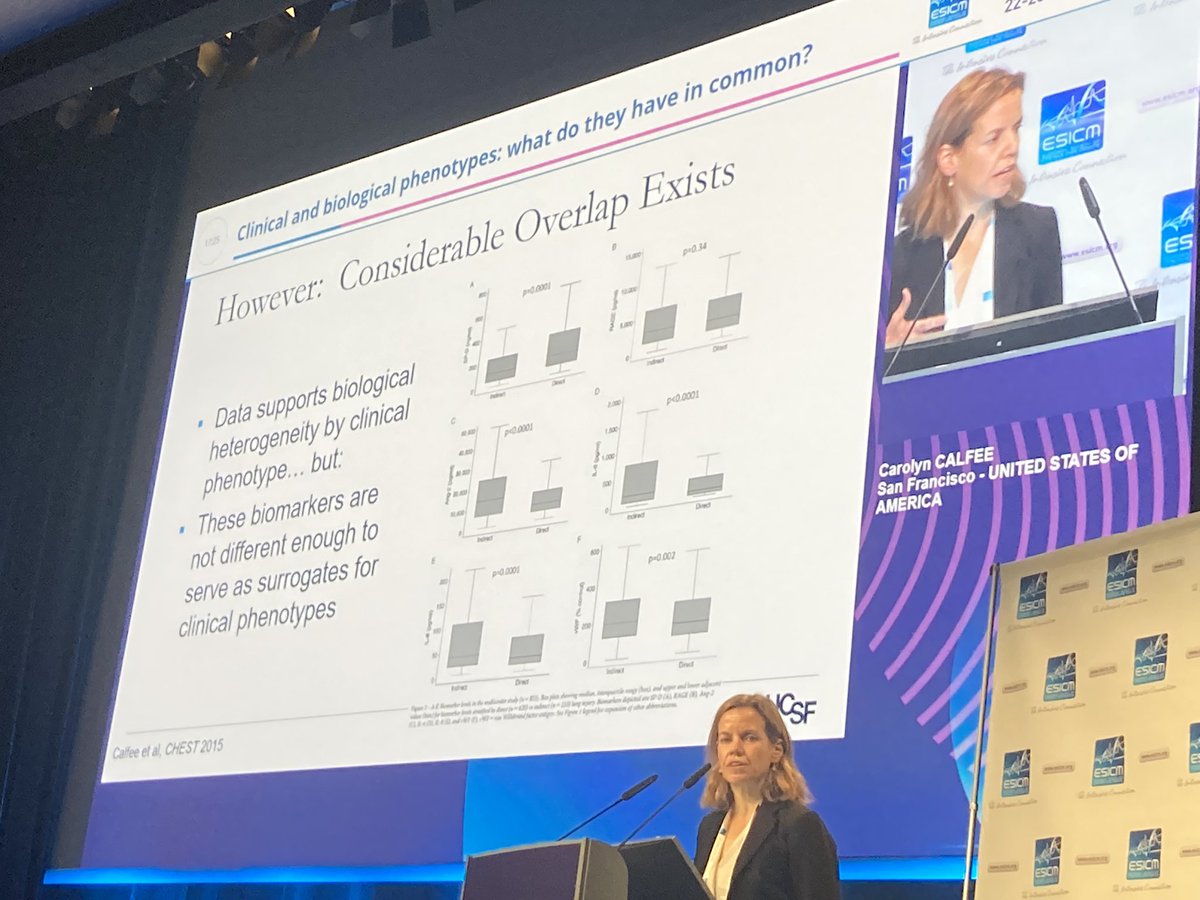
Severe cardiogenic shock has different phenotypes
1. medical cardiogenic shock(AMI, end stage dilated CM, myocarditis, septic shock)
2. Post cardiotomy refractory CS (post CABG)
#LIVES2022
@ESICM #ecmo #resuscitation #ALS
Alain COMBES
Severe cardiogenic shock has different phenotypes
1. medical cardiogenic shock(AMI, end stage dilated CM, myocarditis, septic shock)
2. Post cardiotomy refractory CS (post CABG)
#LIVES2022
@ESICM #ecmo #resuscitation #ALS
@ESICM 2022 what do the guidelines say
- ESC recommends short term MCS should be considred in cardiogenic shock.
IABP may be considered but not routinely recommended in post MI
#LIVES2022
- ESC recommends short term MCS should be considred in cardiogenic shock.
IABP may be considered but not routinely recommended in post MI
#LIVES2022
What about in fulminant!myocarditis ? Mostly giant cell myocarditis #LIVES2022 

What about in cardiomyopathy patients?
- ECMO can be used as a bridge to heart transplant
- the other strategy is "bridge to bridge"
- 2 ecmo device for each L and R heart WOAHHHH!!
- ECMO can be used as a bridge to heart transplant
- the other strategy is "bridge to bridge"
- 2 ecmo device for each L and R heart WOAHHHH!!
2 ecmo for 1 pt

ECMO has completely changed the way we manage heart transplant
- 20 years ago we dont have VA ECMO and not this rapidly
- e.g., RV failure post heart transplant.
- see below where ECMO pre Heart tx has almost as good outcome
- 20 years ago we dont have VA ECMO and not this rapidly
- e.g., RV failure post heart transplant.
- see below where ECMO pre Heart tx has almost as good outcome

Next : what about in life-threatening PE?
this is a difficult area.
timing is very important
- as part of resuscitation OR to stabilise severe haemodynamics OR in case of failed sys thrombolytics or catheter directed therapies.
#pe #massivepe #ecmo #LIVES2022
this is a difficult area.
timing is very important
- as part of resuscitation OR to stabilise severe haemodynamics OR in case of failed sys thrombolytics or catheter directed therapies.
#pe #massivepe #ecmo #LIVES2022
Of course any #ecmo talk won’t be complete without talking ARREST trial. Really good outcome.

Contrast this with Prague OHCA
- non significant outcome.
(massive differences -- @drizopoulos has an ECMO bus that goes to scene, amongst many others) PRague - pt brought to centre.
- AGE and COLLAPSE to ECMO time - KEY
pubmed.ncbi.nlm.nih.gov/35191923/
#ecmo #ecpr #ALS #LIVES2022
- non significant outcome.
(massive differences -- @drizopoulos has an ECMO bus that goes to scene, amongst many others) PRague - pt brought to centre.
- AGE and COLLAPSE to ECMO time - KEY
pubmed.ncbi.nlm.nih.gov/35191923/
#ecmo #ecpr #ALS #LIVES2022
@drizopoulos What about in "septic shock" - niche group
pubmed.ncbi.nlm.nih.gov/32828186/
ECMO patient has higher probability of survival . mortality dropped from 85 to 45%
Hazard ratio of 0.24.
Time window is "very narrow" here too to note.
#ecmo #septicshock #LIVES2022
pubmed.ncbi.nlm.nih.gov/32828186/
ECMO patient has higher probability of survival . mortality dropped from 85 to 45%
Hazard ratio of 0.24.
Time window is "very narrow" here too to note.
#ecmo #septicshock #LIVES2022

But class E may not be the right patient group. Multi organ failure is major risk factors for not surviving Ecmo. We need to find right patient group perhaps in scai C D groups. #LIVES2022 #ecmo #ECMO

A few more trials coming and more results likely to come out soon over next few months and years.
Another trial in France ongoing with a different primary end point.
#LIVES2022
#ECMO #als #resuscitation #mcs
Another trial in France ongoing with a different primary end point.
#LIVES2022
#ECMO #als #resuscitation #mcs
Q: what about using ECMO earlier not as a final rescue device but more commonly?
A: clearly we have to move on to earlier in disease process but we do need to work on early identification of this patient groups for both ecmo and impella
#ecmo #LIVES2022
#ECMO
A: clearly we have to move on to earlier in disease process but we do need to work on early identification of this patient groups for both ecmo and impella
#ecmo #LIVES2022
#ECMO
Q: drug toxicity cardiogenic shock?
A: again if started early could have good outcomes. WE SHOULD NOT hesitate to start ECMO in 2022 -- this is so 2010. :P #ECMO #als #MCS #LIVES2022
A: again if started early could have good outcomes. WE SHOULD NOT hesitate to start ECMO in 2022 -- this is so 2010. :P #ECMO #als #MCS #LIVES2022
@UnrollHelper unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh