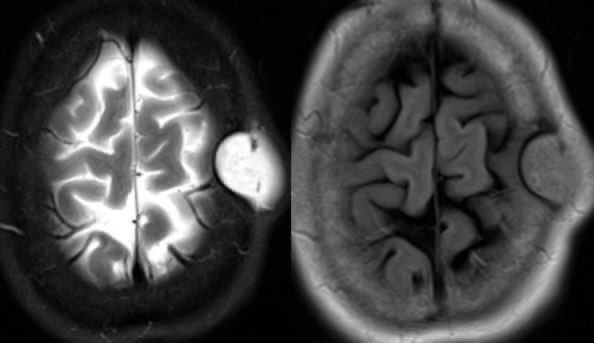
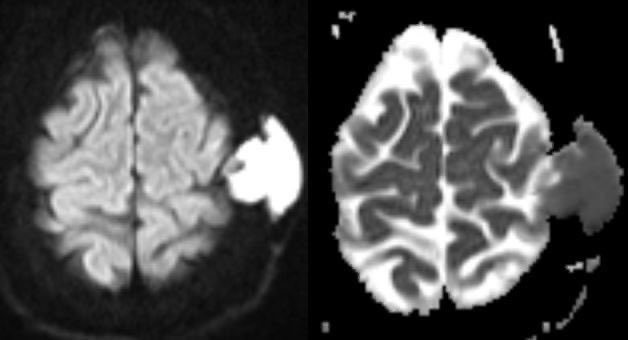
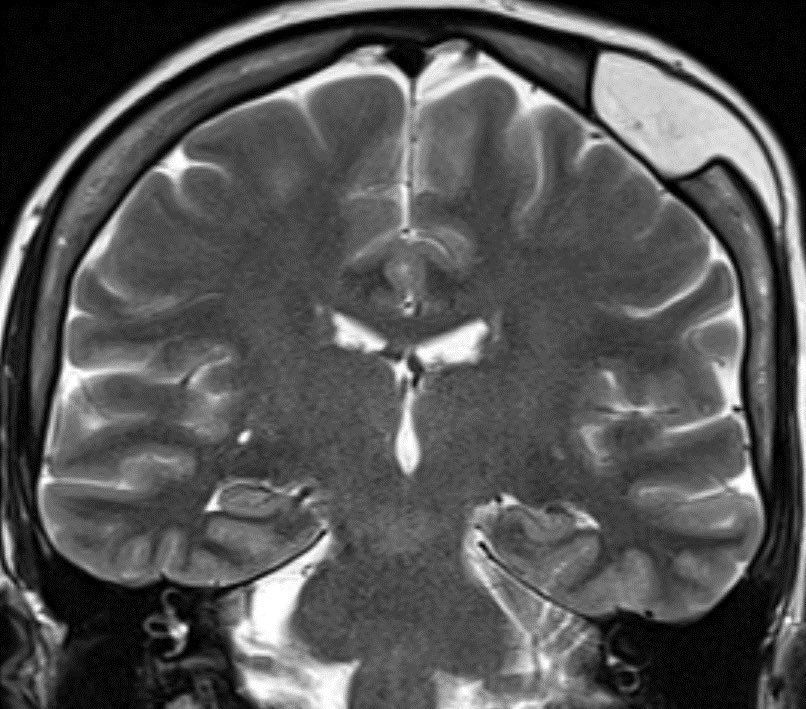
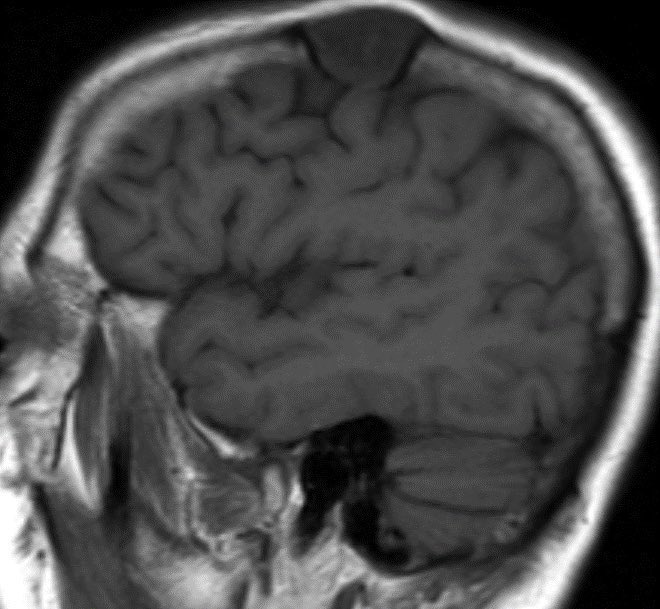
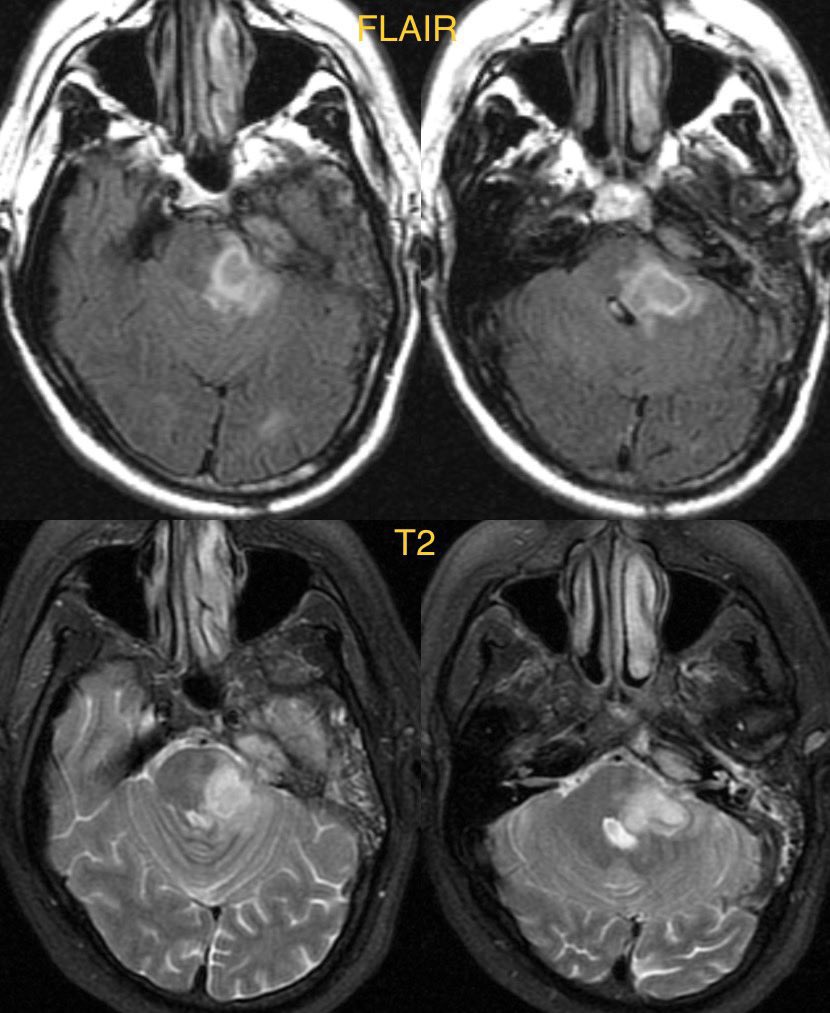
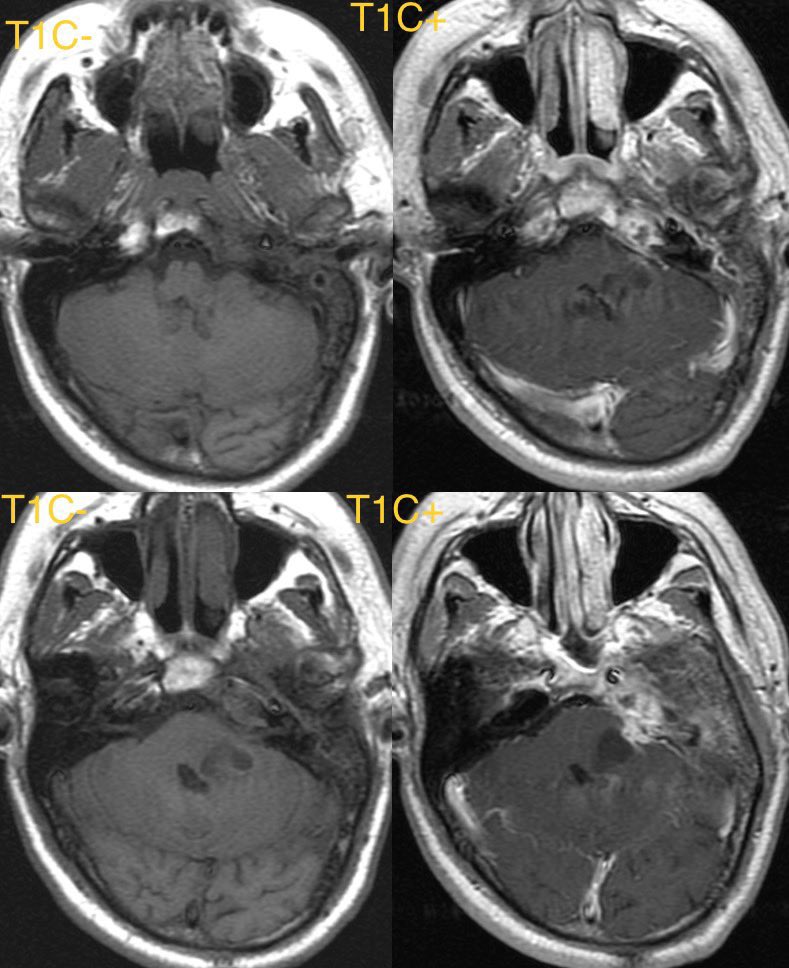
23 yr old with headache. MR shows a “bubbly” mass in the right lateral ventricle near the foramen of Monro. The mass abuts the septum pellucidum and displays mild contrast enhancement.
#neurotwitter #radtwitter #RadEd #MedTwitter #radres @TheASNR @ESNRad @ASHNRSociety
#neurotwitter #radtwitter #RadEd #MedTwitter #radres @TheASNR @ESNRad @ASHNRSociety




Differential diagnosis:
Subependymoma
Choroid plexus neoplasm
Central neurocytoma
Intraventricular meningioma
Mets
Subependymoma
Choroid plexus neoplasm
Central neurocytoma
Intraventricular meningioma
Mets
Answer: confirmed central neurocytoma
Classically, look for the “bubbly” mass abutting/attached to the septum pellucidum near the foramen of monro with enhancement.
#futureradres
Classically, look for the “bubbly” mass abutting/attached to the septum pellucidum near the foramen of monro with enhancement.
#futureradres
• • •
Missing some Tweet in this thread? You can try to
force a refresh