1/Is your ability to remember temporal lobe anatomy seem, well, temporary?
Here’s a #tweetorial to help you remember the structures of the temporal lobe!
#medtwitter #meded #neurotwitter #radtwitter #radres #neurorad #FOAMed #neurosurgery #medstudenttwitter #neurology
Here’s a #tweetorial to help you remember the structures of the temporal lobe!
#medtwitter #meded #neurotwitter #radtwitter #radres #neurorad #FOAMed #neurosurgery #medstudenttwitter #neurology

2/Temporal lobe can be divided centrally & peripherally. Centrally is the hippocampus. It’s a very old part of the brain & is relatively well preserved going all the way back to rats. Its main function is memory—getting both rats & us through mazes—including the maze of life
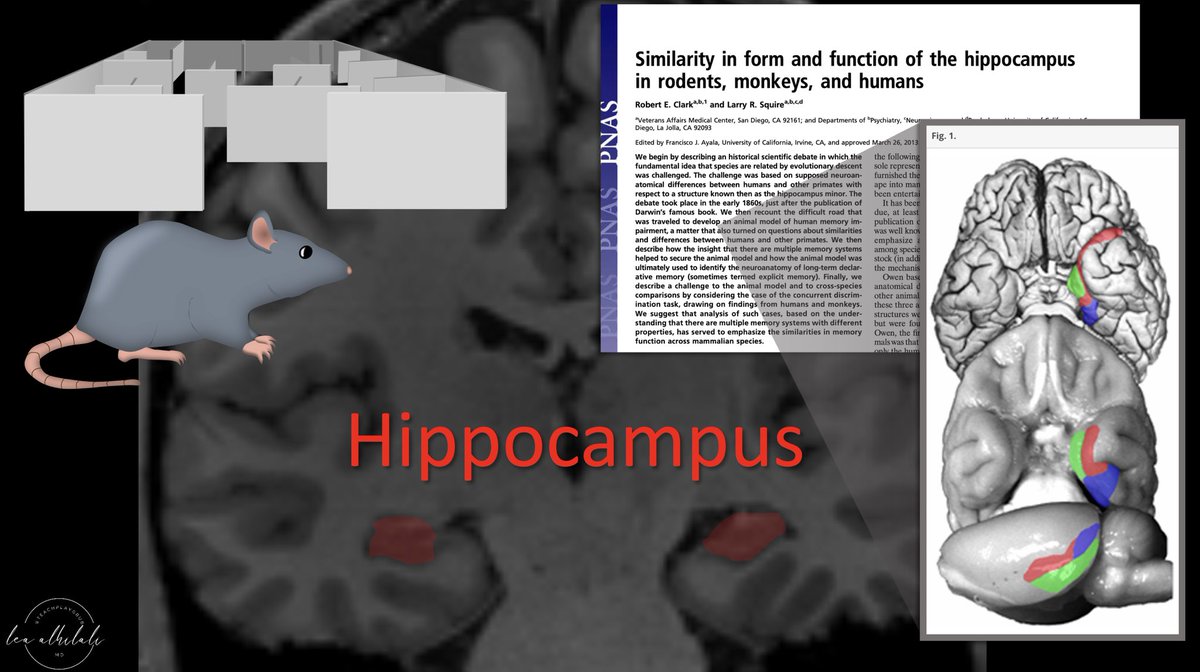
3/Peripherally is the neocortex. Although rats also have neocortex, theirs is much different structurally than humans.
So I like to think of neocortex as providing the newer (neo) functions of the temporal lobes seen in humans: speech, language, visual processing/social cues
So I like to think of neocortex as providing the newer (neo) functions of the temporal lobes seen in humans: speech, language, visual processing/social cues

4/So let’s start w/the oldest part of the temporal lobe, the hippocampus, and we will move clockwise from there.

5/Next to the hippocampus is the parahippocampal gyrus. I remember this b/c the hippocampus is the oldest part of the temporal lobe & older folks love to go in pairs. So this is the PAIR-ahippocampal gyrus—it pairs w/the old hippocampus

6/Next to the parahippocampal gyrus is the fusiform gyrus. I remember this b/c this gyrus bridges (some might say FUSES) the older, allocortex part of the temporal lobe (hippocampus/parahippocampal) w/the newer, neocortical structures. Fusiform gyrus is the neocortical bridge

7/Fusiform gyrus bridges the older temporal lobe w/the new lateral temporal neocortex.
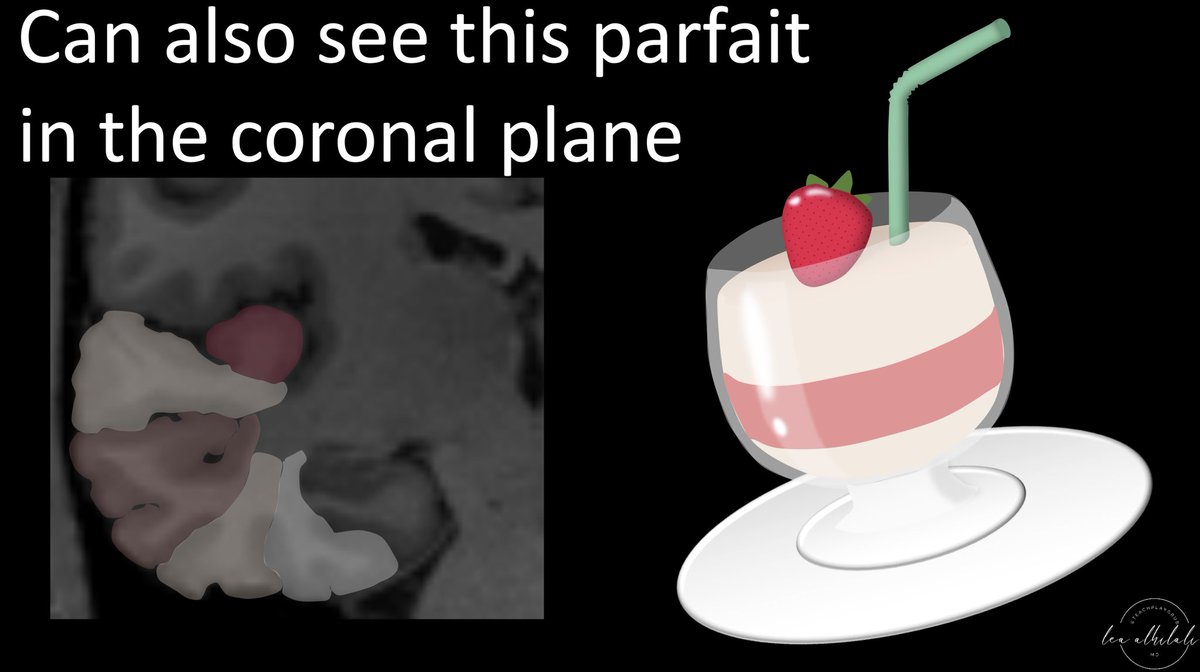
I think the lateral neocortex looks like a parfait—w/the superior, middle, & inferior temporal gyri layered on top of the fusiform gyrus. Heschl’s transverse gyrus forms the strawberry on top
I think the lateral neocortex looks like a parfait—w/the superior, middle, & inferior temporal gyri layered on top of the fusiform gyrus. Heschl’s transverse gyrus forms the strawberry on top

8/You can remember that the fusiform gyrus is at the bottom of this parfait b/c fusiform means elongated—and the stem of a parfait glass is elongated—almost fusiform!

9/You can remember that Heschl’s gyrus is the fruit on top b/c Heschl sounds like Bushel, and fruit to put on top comes in Bushels!

10/You can also see this parfait in the coronal plane, although it is a little tilted!
11/Last temporal lobe structure is the temporal stem. It is the white matter connecting the gyri of the temporal lobe to the rest of the brain. I remember this b/c I think the temporal lobe looks like an upside-down cauliflower—& the STEM of that cauliflower is the temporal STEM

12/So now you can remember the anatomy of the temporal lobe:
An old couple
A bridge fusing them to the next generation
A delicious parfait
All connected by a cauliflower stem.
I hope this new anatomy knowledge will be anything but temporary!
An old couple
A bridge fusing them to the next generation
A delicious parfait
All connected by a cauliflower stem.
I hope this new anatomy knowledge will be anything but temporary!

• • •
Missing some Tweet in this thread? You can try to
force a refresh