Important news about XXB1.5 pointing out that infection is more via the ACE2 receptor than previous Omicron variants.
But … the mouth is not mentioned as an important site of infection…. cambridgeindependent.co.uk/news/fast-spre…
A thread … 1/
But … the mouth is not mentioned as an important site of infection…. cambridgeindependent.co.uk/news/fast-spre…
A thread … 1/
2/ Minor salivary glands over the surface of the tongue, inner surface of the lips, the fauces and soft palate are highly susceptible to infection and replication. Epithelial cells in these areas express the ACE2 receptor.
nature.com/articles/s4159…
nature.com/articles/s4159…
3/ The mouth can be considered a viral factory with viral entry into saliva in high quantity - 100 million per ml (equivalent to half a billion viruses in a single 5 ml teaspoon). ncbi.nlm.nih.gov/pmc/articles/P…
4/ Importantly, contrary to common perception - as expressed in the Cambridge Independent article above - the airways of the lungs do not express the ACE2 receptor in high intensity. It is found in nasal airways 200-700 x more intensely… erj.ersjournals.com/content/56/3/2…
5/ And the ACE2 receptor is not found in the airways of the lungs in normal individuals… embopress.org/doi/full/10.15…
6/ The target organ for #SARS2 is not the lungs, at least not the airways. Yes the lungs are damaged but it is the blood vessels which take the hit, the airways are not inflamed (totally unlike influenza). See this presentation from Nov 2020.
7/ And this hypothesis proposed that viral transfer to the lungs is via the bloodstream, worsened in those with poor oral health (gum disease / periodontitis) with viral interaction with the lung endothelium ACE2 leading to the lung damage. genesispub.org/resource/image… 

8/ The endothelium (the inner lining of all blood vessels in the body) is the site of damage by #SARS. This is as much true for the lungs as for other tissues and organs. nature.com/articles/s4140…
9/ A reminder that poor oral health is massively associated with poor outcome. If you have severe gum disease (you may not be aware that you do) then there is an approx 8-fold risk of death. pubmed.ncbi.nlm.nih.gov/33527378/
10/ The mouth should be seen as an immune organ and if you have poor oral health then you should be considered immune compromised in relation to #COVID.
11/ Here is a presentation to explain in more detail …
12/ High viral load (the number of viruses) in the mouth is reported as a better predictor of death than the patient’s age. And this is independent of nasopharyngeal viral load… medrxiv.org/content/10.110…
13/ And there is something we can potentially do about it. This study shows reduced length of stay in hospital, reduced ITU admission and reduced death simply by adding a mouthwash which reduces viral load in the mouth. nature.com/articles/s4159…
14/ The mouthwash in that study is not available outside Brazil. At our hospital we use a mouthwash containing CPC (cetylpyridinium chloride) which is probably the best ingredient for killing #SARS2 in the mouth. I was interview on this by @LindsayDixonFP5
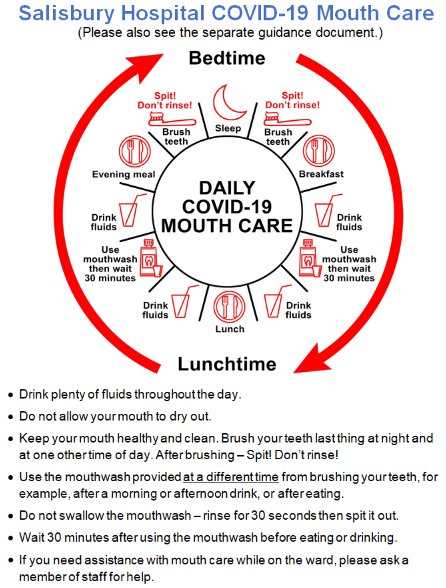
15/ Here is our current patient information guidance @SalisburyNHS (awaiting update) salisbury.nhs.uk/coronavirus/co…
16/ Please note this is not all about mouthwash. It is about oral health generally and taking the best care possible of your mouth (please ask your dentist for advice - if you can find one).
17/ The long term health implications for poor oral health are massive.
Oral organisms evidently cause or worsen important diseases of the body.
Here is a more in-depth presentation - start watching at 28:18
Oral organisms evidently cause or worsen important diseases of the body.
Here is a more in-depth presentation - start watching at 28:18
18/ There is now a growing awareness of the links between poor oral health and general health. I am pleased to collaborate with colleagues in the world of dentistry and periodontology to further understanding.
19/ In the meantime please understand that the mouth plays a key part of disease development and viral transmission in the context of #COVID.
20/ I am pleased to say I’m working with collaborators in the UK to find out what is going on in the mouth in #longCOVID with a pilot study which started this week.
21/ Also pleased to be working with #teamclots to further our understanding of the role of the endothelium, platelet activation and microclots in those with #longCOVID.
I think understanding the anatomical playing field will be important (as is the case for all diseases).
I think understanding the anatomical playing field will be important (as is the case for all diseases).
22/ Off to brush my teeth …
• • •
Missing some Tweet in this thread? You can try to
force a refresh