
You are again asked to see a patient with GBS. A young man in his 30's, does not seem perturbed by his acute onset of weakness of lower limbs. He says he has been through it on many occasions before. This particular bout was triggered after a hearty meal at a wedding. Thoughts?
An important differential to GBS are the Channelopathies. This gentleman had low levels of Potassium, and correction of the same completely reversed his symptoms! On evaluation, he was diagnosed with a Channelopathy
Simplified Approach
#Neurology
Simplified Approach
#Neurology

Hypokalaemia is notorious to cause neurological weakness often mimicking GBS. However clinical pointers for it are
- Recurrent Attacks
- Triggered by Alcohol/Carbs
- No Bulbar/ Facial Involvement
-Preserved reflexes (Can have areflexia!)
-Rapid (to come and go)
-Normal CSF
- Recurrent Attacks
- Triggered by Alcohol/Carbs
- No Bulbar/ Facial Involvement
-Preserved reflexes (Can have areflexia!)
-Rapid (to come and go)
-Normal CSF
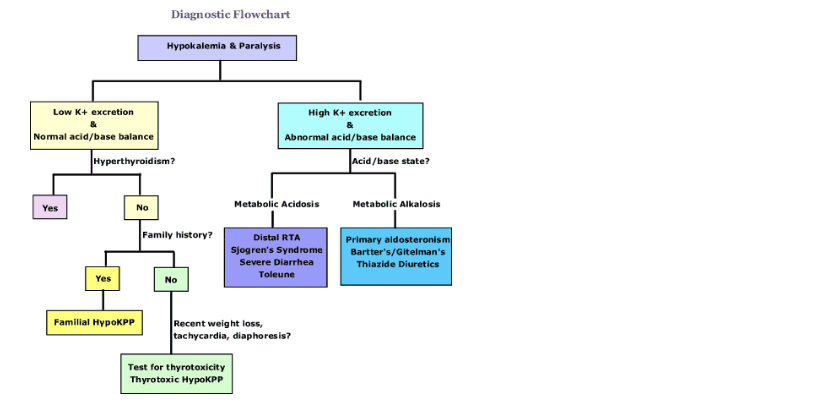
Hypokalaemia may be due to a primary Channelopathy, which are rare diseases, for more commonly secondary to an underlying cause of hypokalaemia. So in a patient with HypoK paralysis:-
Step 1: Is there any Acid Base Abnormality?
If NO -> think of the primary channelopathies
If YES
Step 2:
Metabolic Acidosis:
Distal RTA (eg Sjogren's: have seen a number of such patients!)
Diarrhea
Metabolic Alkalosis:
Hyperaldosteronism
Bartter/Gitelman
Thiazide Use
If NO -> think of the primary channelopathies
If YES
Step 2:
Metabolic Acidosis:
Distal RTA (eg Sjogren's: have seen a number of such patients!)
Diarrhea
Metabolic Alkalosis:
Hyperaldosteronism
Bartter/Gitelman
Thiazide Use
Secondary causes are most common, hence ask for
Dry Eyes/Mouth, arthralgia (Sjogren)
GI disturbances
Hypertension in Young
Detailed Drug history
Dry Eyes/Mouth, arthralgia (Sjogren)
GI disturbances
Hypertension in Young
Detailed Drug history
Coming to the Channelopathies
Theseinclude :
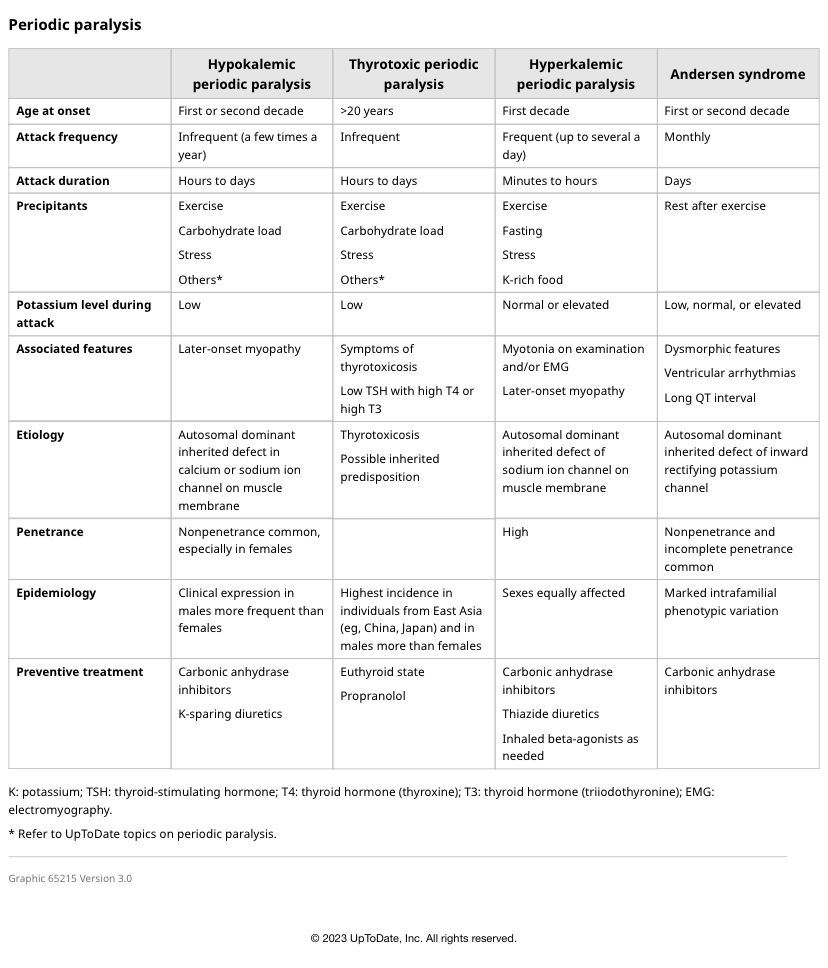
1. Hypokalemic Periodic Paralysis (Calcium Channel)
2. Hyperkalemic Periodic Paralysis (Sodium Channel)
3. Anderson Tawil Syndrome (Potassium Channel)
4. Thyrotoxic Periodic Paralysis (Potassium Channel) (most common in India)
Theseinclude :
1. Hypokalemic Periodic Paralysis (Calcium Channel)
2. Hyperkalemic Periodic Paralysis (Sodium Channel)
3. Anderson Tawil Syndrome (Potassium Channel)
4. Thyrotoxic Periodic Paralysis (Potassium Channel) (most common in India)
Hypokalemic Periodic Paralysis
- Recurrent episodes
- triggered by high carb diet/alcohol
- can eventually progress to a fixed weakness
Rx: Acetazolamide, Spironolactone Potassium Supplement Avoid High Carb/alcohol
- Recurrent episodes
- triggered by high carb diet/alcohol
- can eventually progress to a fixed weakness
Rx: Acetazolamide, Spironolactone Potassium Supplement Avoid High Carb/alcohol
Hyperkalemic Periodic Paralysis
More frequent and shorter attacks
MYOTONIA is present
Triggered by fasting (Contrast with hypo)
Cardiac involvement (high K)
Rx: Glucose / Calcium
Caveat: Potassium Levels can be normal when tested, so normal K does not rule out the diagnosis
More frequent and shorter attacks
MYOTONIA is present
Triggered by fasting (Contrast with hypo)
Cardiac involvement (high K)
Rx: Glucose / Calcium
Caveat: Potassium Levels can be normal when tested, so normal K does not rule out the diagnosis
Andersen Tawil Syndrome
1. Episodic Weakness
2. Ventricular Arrythmias
3. Dysmorphic Facies
1. Episodic Weakness
2. Ventricular Arrythmias
3. Dysmorphic Facies
Thyrotoxic Periodic Paralysis
Basically via Hypokalemia, so similar features
May have evidence of Thyrotoxicosis
Drug of Choice: Beta Blocker/Propranolol
Basically via Hypokalemia, so similar features
May have evidence of Thyrotoxicosis
Drug of Choice: Beta Blocker/Propranolol
Coming to our patient
No cranial nerve inv.
Recurrent symptoms, triggered by heavy meal, low potassium level prompted suspicion of Hypokalaemia.
No Acid Base Abn]
Sketchy family history of similar complaints
No evidence of myotonia, sicca, GI abnormalities, HTN
Thyroid:Normal
No cranial nerve inv.
Recurrent symptoms, triggered by heavy meal, low potassium level prompted suspicion of Hypokalaemia.
No Acid Base Abn]
Sketchy family history of similar complaints
No evidence of myotonia, sicca, GI abnormalities, HTN
Thyroid:Normal
Potassium corrected and he is discharged on Acetazolamide, and counselled about diet/alcohol
So far no recurrences !
So far no recurrences !
Here is yet another mimic of GBS! Every patient with GBS should be evaluated for this. It is a lot more common than we realise, and easy amenable to treatment, indeed, so one may be more cautious for a deadly arrhythmia
#MedTwitter #MedEd #NeuroTwitter
#MedTwitter #MedEd #NeuroTwitter
Src: hkpp.org
From UpToDate
• • •
Missing some Tweet in this thread? You can try to
force a refresh











