The history of methotrexate began 75 years ago.
A short 🧵 on its history and pivotal moments, covering key trials to show realignment of #hematology #rheumatology, disciplines that belong to each other♥️
#MedTwitter
A short 🧵 on its history and pivotal moments, covering key trials to show realignment of #hematology #rheumatology, disciplines that belong to each other♥️
#MedTwitter

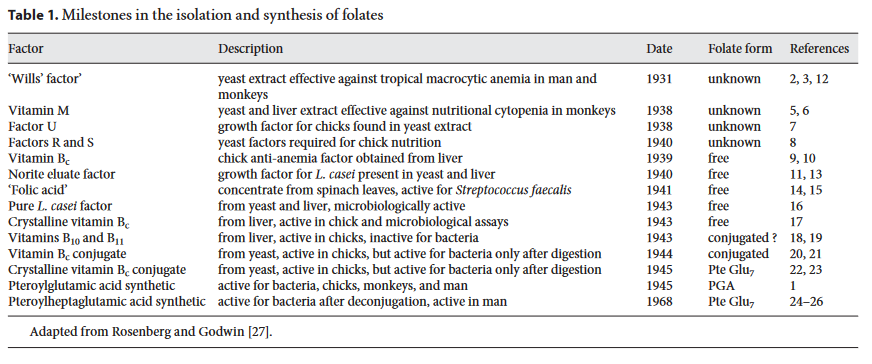
In the early 1940s, folic acid was isolated and found to cure some patients with megaloblastic anemia, not responding to vitamin B 12.
Also, patients with acute leukemia were treated with folic acid or folate conjugates (polyglutamated forms of folic acid)
👉proved ineffective:(
Also, patients with acute leukemia were treated with folic acid or folate conjugates (polyglutamated forms of folic acid)
👉proved ineffective:(

The subsequent demonstration by Heinle and Welch that a diet-induced deficiency of folic acid caused a decrease in the leukemia cell count, stimulated efforts, primarily by the Lederle group, to synthesize analogs of folic acid.
Overview of isolation and synthesis of folates👇
Overview of isolation and synthesis of folates👇
Era of chemotherapy:
-Aminopterin (4-aminopterolylglutamic acid),
proved to be a powerful antagonist, shown by Farber et al in a landmark paper, to produce remissions in children with acute lymphocytic leukemia (ALL)
-nitrogen mustard caused regressions in patients with lymphoma
-Aminopterin (4-aminopterolylglutamic acid),
proved to be a powerful antagonist, shown by Farber et al in a landmark paper, to produce remissions in children with acute lymphocytic leukemia (ALL)
-nitrogen mustard caused regressions in patients with lymphoma

Aminopterin interfered with proliferation of connective tissue. This led to a study in 1951 by Gubner et al. in several patients with rheumatoid arthritis, psoriasis, and psoriatic arthritis👉rapid improvement in RA signs and symptoms 6/7 seven patients

In 1956, studies of leukemia-bearing mice showed that methotrexate, another folate analog, had a therapeutic index superior to that of´aminopterin; based on these studies, methotrexate supplanted
aminopterin in the clinic.
aminopterin in the clinic.
Lessons learnt early:
-drug resistance occurs rapidly if cure is not achieved (for most tumors within 4-6 months)👉treatment failure
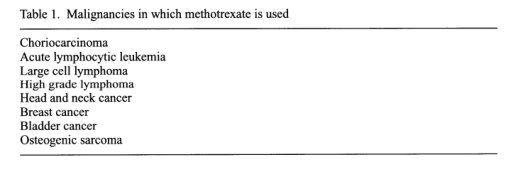
-curable diseases with drugs: Hodgkin's, DLBCL, certain childhood solid tumors
-treatment with MTX not associated with long term
side effects
-drug resistance occurs rapidly if cure is not achieved (for most tumors within 4-6 months)👉treatment failure
-curable diseases with drugs: Hodgkin's, DLBCL, certain childhood solid tumors
-treatment with MTX not associated with long term
side effects
Other drugs were also found to be useful in the treatment of ALL, in particular 6-mercaptopurine (6MP), prednisone, and vincristine.
A very important study by the Acute Leukemia B cooperative group showed that 6MP-MTX was better than either drug used alone.
A very important study by the Acute Leukemia B cooperative group showed that 6MP-MTX was better than either drug used alone.

The next major advance (1971, 1978) that led to cures in 50% of the patients was the use of intrathecal methotrexate with adequate central nervous system (CNS) irradiation, for prophylaxis of sanctuary disease.

In 1972, Rex Hoffmeister, reported positive effects with intramuscular MTX (10-15 mg per week) in 29 patients with RA. 11/2929 patients had “major” clinical improvements and 14 had “moderate” improvements in RA activity. These patients underwent treatment for up to 25 months.

In 1983, a RCT crossover study of 35 patients with refractory RA was done.
Initial MTX dose: 7.5 mg per week with an increase at 6 weeks to 15 mg/w.
- 3 weeks after MTX initiation: >50% with >50% improved joint tenderness index
- 39% with improvement in the joint swelling index
Initial MTX dose: 7.5 mg per week with an increase at 6 weeks to 15 mg/w.
- 3 weeks after MTX initiation: >50% with >50% improved joint tenderness index
- 39% with improvement in the joint swelling index

The other pivotal study was an NIH-funded study network of 189 patients with active RA. Patients initially received MTX at 7.5 mg per week with dose escalation to 15 mg per week.
-32% had >50% decrease in the joint tenderness index
-21% with reduction in joint swelling index
-32% had >50% decrease in the joint tenderness index
-21% with reduction in joint swelling index

Graft-versus-host disease:
In 1986, Storb and colleagues reported that the combination of MTX with cyclosporine A was superior to CSA alone in a series of prospective randomized phase 3 trials. This remains one of the most widely used regimen today as prophylaxis regimen in BMT.
In 1986, Storb and colleagues reported that the combination of MTX with cyclosporine A was superior to CSA alone in a series of prospective randomized phase 3 trials. This remains one of the most widely used regimen today as prophylaxis regimen in BMT.

If we go back in time 75 years and tell Dr Farber, that 21st-century medicine would utilize MTX more in rheumatology but also show the widespread use in oncology and hematology, he might scratch his head...that's a lovely thought, showing the beauty of medical research!
Fin.
Fin.

Sources and references:
ncbi.nlm.nih.gov/pmc/articles/P…
ashpublications.org/blood/article/…
nejm.org/doi/pdf/10.105…
pubmed.ncbi.nlm.nih.gov/14799481/
karger.com/Article/Abstra…
onlinelibrary.wiley.com/doi/epdf/10.10…
ncbi.nlm.nih.gov/pmc/articles/P…
ashpublications.org/blood/article/…
nejm.org/doi/pdf/10.105…
pubmed.ncbi.nlm.nih.gov/14799481/
karger.com/Article/Abstra…
onlinelibrary.wiley.com/doi/epdf/10.10…
• • •
Missing some Tweet in this thread? You can try to
force a refresh