How my half day work ✂️ on a Saturday is progressing…😄
1. Young lady with 🫀 disease referred by ENT doc with epistaxis 👃
1. Young lady with 🫀 disease referred by ENT doc with epistaxis 👃



Pounding heart 💓 with loud P2 & PSM at the lower left sternal area
I got the mother and she said since 6 months she is blue 🔵
Centralcyanosis➕Clubbing➕VSD➕PulmHTN
There was Hx of recurrent LRTIs in childhood.
I got the mother and she said since 6 months she is blue 🔵
Centralcyanosis➕Clubbing➕VSD➕PulmHTN
There was Hx of recurrent LRTIs in childhood.

I sent her 🏠 to get old records 🔖 and our suspicion of cyanotic CHD with incd 🫁 blood flow due to TOGV was right 🫵🏽

Her CBC proved why she’s having epistaxis 🩸
She’s having secondary polycythemia with erythrocytosis causing hyperviscosity symptoms ☄️
She’s having secondary polycythemia with erythrocytosis causing hyperviscosity symptoms ☄️

Sadly nothing could be done for her 😓now that she has developed Eisenmenger syndrome 🌒 and her heart disease is so progressed to offer her any corrective surgery at this age😧
2. Just when I am abt to leave for lunch 🥗, a man came in ED with history of falling from his 🚲 and refused admission in 2 hospitals coz of no BP & pulse 😪
Told my staff to do ECG and that made sure I am in for the long exciting day 😬
Told my staff to do ECG and that made sure I am in for the long exciting day 😬
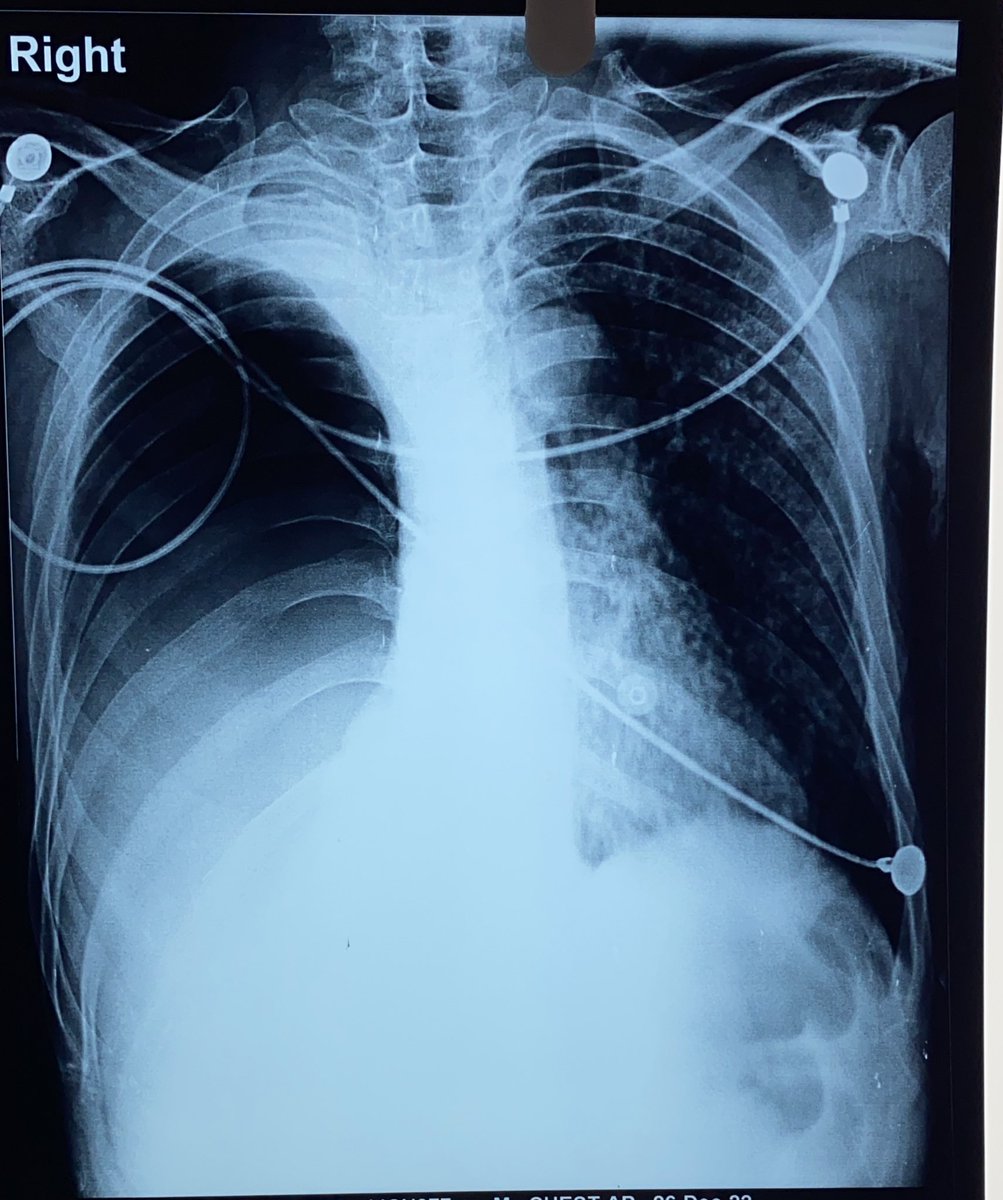
64 yr old 👳♂️ with no DM or HTN or 🚬 or 🍺 history , but chews tobacco had a syncope with severe cardiogenic shock ⚡️
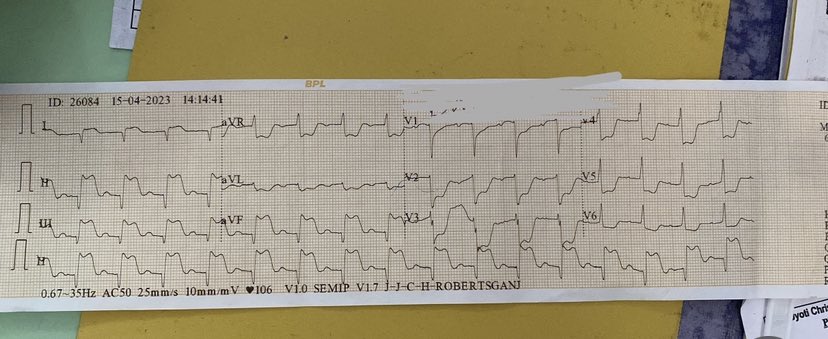
ECG showed ST elevation 📈 in inferior leads.
We loaded the STK 💉 & as we were giving loading doses of DAPT➕ high intensity statins, he had this 👇
ECG showed ST elevation 📈 in inferior leads.
We loaded the STK 💉 & as we were giving loading doses of DAPT➕ high intensity statins, he had this 👇
This is ST elevation inferior wall MI with complete heart block 🚫
This is bad 👎 and confers bad prognosis for the MI 😑
We gave him one shot of Atropine 🩼 and started Dopamine infusion
We gave plenty of iv fluids 💦 and monitored his urine output 🚰
This is bad 👎 and confers bad prognosis for the MI 😑
We gave him one shot of Atropine 🩼 and started Dopamine infusion
We gave plenty of iv fluids 💦 and monitored his urine output 🚰
With the thrombolysis and other Rx, rhythm normalised 🤗 and he is symptomatically better 👍
His repeat ECG also reassured us 👇 with less ST elevation and SR of 80 rate 😇
Jesus has been kind to our efforts 🙏
His repeat ECG also reassured us 👇 with less ST elevation and SR of 80 rate 😇
Jesus has been kind to our efforts 🙏

3. Just when I was taking a breather, my JMO said one 18 yr old👦 who’s pale like a ⚪️ paper has come ☹️
Seeing his hemolytic face,feeling his big spleen & hearing from his father that his sister 👧 has a blood disease for which many 🩸 transfusions have been given,I knew this…
Seeing his hemolytic face,feeling his big spleen & hearing from his father that his sister 👧 has a blood disease for which many 🩸 transfusions have been given,I knew this…
… is Sickle Cell Anemia
On asking more, he has been havg painful episodes in his 🦵➕chest for which many 🥼 have given him analgesic 💉
Nobody bothered to make the connection with his sister’s sickle cell disease 😧
No wonder SCA is a neglected disease and remains so 😰
On asking more, he has been havg painful episodes in his 🦵➕chest for which many 🥼 have given him analgesic 💉
Nobody bothered to make the connection with his sister’s sickle cell disease 😧
No wonder SCA is a neglected disease and remains so 😰
His CBC showed severe anemia, thrombocytopenia ➕ hemolytic markers were ⬆️—LDH 673, retics 6%, IB 2.5
Maybe he’s thalassemia trait with HbS heterozygous state as it’s a microcytic hypochromic anemia which never required transfusion 😯
Maybe he’s thalassemia trait with HbS heterozygous state as it’s a microcytic hypochromic anemia which never required transfusion 😯

He was administered Tramadol and Diclofenac injection for his pain and blood was mobilised
I convinced his 👨 to send HPLC & get his daughter’s treatment reports📄
I was amazed by the way BHU, Varanasi has treated her and followed her up so far 🫡
Kudos 👏
I convinced his 👨 to send HPLC & get his daughter’s treatment reports📄
I was amazed by the way BHU, Varanasi has treated her and followed her up so far 🫡
Kudos 👏

As I walk back to my 🏡 for a late lunch, I am grateful to God for the opportunities we have as a mission 🏥 to treat these precious patients 🤗
Life of a peripheral hospital physician 👨⚕️ is never boring and has immense potential to serve a suffering population 🎭
Life of a peripheral hospital physician 👨⚕️ is never boring and has immense potential to serve a suffering population 🎭
@threadreaderapp unroll pls
• • •
Missing some Tweet in this thread? You can try to
force a refresh