
PICC line 🧵 #medicine
1/
A central device (i.e in the SVC) placed via a peripheral venous access
.
#irad #vascular #MedTwitter #FOAMed #hematology #Tweetorials @nihardesai7 @MedTweetorials #Cardiology #MedEd #oncology #internalmedicine @BrownJHM #MedStudentTwitter #cardiotwitter
1/
A central device (i.e in the SVC) placed via a peripheral venous access
.
#irad #vascular #MedTwitter #FOAMed #hematology #Tweetorials @nihardesai7 @MedTweetorials #Cardiology #MedEd #oncology #internalmedicine @BrownJHM #MedStudentTwitter #cardiotwitter


2/
Classically placed in the arm
May be placed in the leg (eg in #pediatrics /neonates – which may then terminate in the infrarenal IVC/iliacs)
.
#criticalcare #cardiovascular
Classically placed in the arm
May be placed in the leg (eg in #pediatrics /neonates – which may then terminate in the infrarenal IVC/iliacs)
.
#criticalcare #cardiovascular
3/
Advantages:
- Lower infection rate then central lines
- Used in the outpatient setting
- Can be used for several weeks to months
- Duration of PICC lines may be from 4 weeks to 6 months
(although they have been known to be functional for more than 300 days)
Advantages:
- Lower infection rate then central lines
- Used in the outpatient setting
- Can be used for several weeks to months
- Duration of PICC lines may be from 4 weeks to 6 months
(although they have been known to be functional for more than 300 days)
4/
Disadvantages:
- Usually smaller bore, which is less useful for frequent blood draws
- Generally dont last >6 months unlike ports/tunnelled catheters
Disadvantages:
- Usually smaller bore, which is less useful for frequent blood draws
- Generally dont last >6 months unlike ports/tunnelled catheters
5/
Indications:
- Long term antibiotics
- Chemo/vasoactive drug infusions
- Frequent blood withdrawals
- Pts with limited peripheral access
- Rapid infusions
- Delivery of hyperosmolar solutions/TPN
Indications:
- Long term antibiotics
- Chemo/vasoactive drug infusions
- Frequent blood withdrawals
- Pts with limited peripheral access
- Rapid infusions
- Delivery of hyperosmolar solutions/TPN
6/
Contraindications: There are no absolute C/I
Relative C/I:
Burns, trauma, skin infections, H/O venous thrombosis, active bacteremia, sepsis, prior mastectomy/LN dissection, SVC syndrome/central vein thrombosis
Contraindications: There are no absolute C/I
Relative C/I:
Burns, trauma, skin infections, H/O venous thrombosis, active bacteremia, sepsis, prior mastectomy/LN dissection, SVC syndrome/central vein thrombosis
7/
May be Valved/valveless, coated/medicated, Single/double/triple lumen
Preference of venous access: Generally, right arm preferred due to shorter and straighter course to the SVC
Preference: Basilic > median cubital > cephalic > brachial > axillary vein access
May be Valved/valveless, coated/medicated, Single/double/triple lumen
Preference of venous access: Generally, right arm preferred due to shorter and straighter course to the SVC
Preference: Basilic > median cubital > cephalic > brachial > axillary vein access
8/
Basilic vein access:
Generally preferred due to large size, superficial location, straight course, least number of valves and adequate angle for insertion
Basilic vein access:
Generally preferred due to large size, superficial location, straight course, least number of valves and adequate angle for insertion
9/
Median Cubital vein access:
Easily seen as it enters into the basilic vein
However, given its location in the antecubital fossa, constant bending at the elbow increase the risk of complications such as mechanical phlebitis.
Median Cubital vein access:
Easily seen as it enters into the basilic vein
However, given its location in the antecubital fossa, constant bending at the elbow increase the risk of complications such as mechanical phlebitis.
10/
Cephalic vein Access:
Generally less preferred since other than being smaller than the basilic vein, its course through the upper arm can be very tortuous. PICCs placed through this vein are thought to have a higher incidence of mechanical phlebitis.
Cephalic vein Access:
Generally less preferred since other than being smaller than the basilic vein, its course through the upper arm can be very tortuous. PICCs placed through this vein are thought to have a higher incidence of mechanical phlebitis.
11/
Brachial vein:
Advantages: larger size; less frequently thrombosed
Disadvantages: Runs deeper than the basilic vein. Courses close to the brachial artery & median nerve, & therefore, it usually requires ultrasound guidance for access. Risk of intra-procedural arterial trauma
Brachial vein:
Advantages: larger size; less frequently thrombosed
Disadvantages: Runs deeper than the basilic vein. Courses close to the brachial artery & median nerve, & therefore, it usually requires ultrasound guidance for access. Risk of intra-procedural arterial trauma
12/
Technique:
#USG guidance improves outcomes
Steps: Tourniquet > Identify the vein on USG > Seldinger technique:21-22 G needle 0.18 wire > Confirm wire on USG or Fluoro > Insert dilator & introducer sheath > Remove wire & dilator > Insert PICC line > Remove the peelaway sheath
Technique:
#USG guidance improves outcomes
Steps: Tourniquet > Identify the vein on USG > Seldinger technique:21-22 G needle 0.18 wire > Confirm wire on USG or Fluoro > Insert dilator & introducer sheath > Remove wire & dilator > Insert PICC line > Remove the peelaway sheath
13/
Infection rates:
OPD: 1.1/1000 PICC days
IPD: 2.1/1000 PICC days
Infection rates higher for those placed in the antecubital fossa
Prophylacic antibiotics NOT recommended
Infection rates:
OPD: 1.1/1000 PICC days
IPD: 2.1/1000 PICC days
Infection rates higher for those placed in the antecubital fossa
Prophylacic antibiotics NOT recommended
14/
Reasons for removal of PICC
Exit-site and tunnel infections, septicemia, fungemia, septic thrombosis, endocarditis, osteomyelitis and sepsis with signs of shock, and/or end-organ dysfunction are all indications for device removal.
Reasons for removal of PICC
Exit-site and tunnel infections, septicemia, fungemia, septic thrombosis, endocarditis, osteomyelitis and sepsis with signs of shock, and/or end-organ dysfunction are all indications for device removal.
15/
Malposition of PICC
Primary malposition: When malposition occurs upon insertion
Secondary : catheter tip migrates spontaneously after initial placement in a proper location
May require removal, exchange, reposition
Malposition of PICC
Primary malposition: When malposition occurs upon insertion
Secondary : catheter tip migrates spontaneously after initial placement in a proper location
May require removal, exchange, reposition
16/
Complications:
- Catheter damage, line disconnection/fracture
- Malposition
- Cardiac arrhythmias (pull back)
- Air embolism: due to inability to maintain a closed system between the catheter and vasculature
- Phlebitis and infiltration: PICC removal is generally not needed
Complications:
- Catheter damage, line disconnection/fracture
- Malposition
- Cardiac arrhythmias (pull back)
- Air embolism: due to inability to maintain a closed system between the catheter and vasculature
- Phlebitis and infiltration: PICC removal is generally not needed
17/
Thrombotic Causes of Cather Occlusion: Catheter tip high in the SVC has an increased risk of thrombosis (up to 78%).
Other risk factors include >1 insertion attempt, vessel wall damage from previous catheter placement, left-sided insertion, and triple lumen catheters.
Thrombotic Causes of Cather Occlusion: Catheter tip high in the SVC has an increased risk of thrombosis (up to 78%).
Other risk factors include >1 insertion attempt, vessel wall damage from previous catheter placement, left-sided insertion, and triple lumen catheters.
18/
Non thrombotic causes of PICC occlusion: Catheter abutment against the wall of a vessel or kinking
Drugs can cause blockage: Common drugs known to precipitate are etoposide, calcium, diazepam, phenytoin, heparin and total parenteral nutrition
Non thrombotic causes of PICC occlusion: Catheter abutment against the wall of a vessel or kinking
Drugs can cause blockage: Common drugs known to precipitate are etoposide, calcium, diazepam, phenytoin, heparin and total parenteral nutrition
19/
Ideal PICC line position:
Tip at cavo-atrial junction
Right 3rd anterior IC space on CXR
2 vertebral bodies below carina (T5-T6 level)
Point of right bronchus intermedius crossing the right heart border
Ideal PICC line position:
Tip at cavo-atrial junction
Right 3rd anterior IC space on CXR
2 vertebral bodies below carina (T5-T6 level)
Point of right bronchus intermedius crossing the right heart border

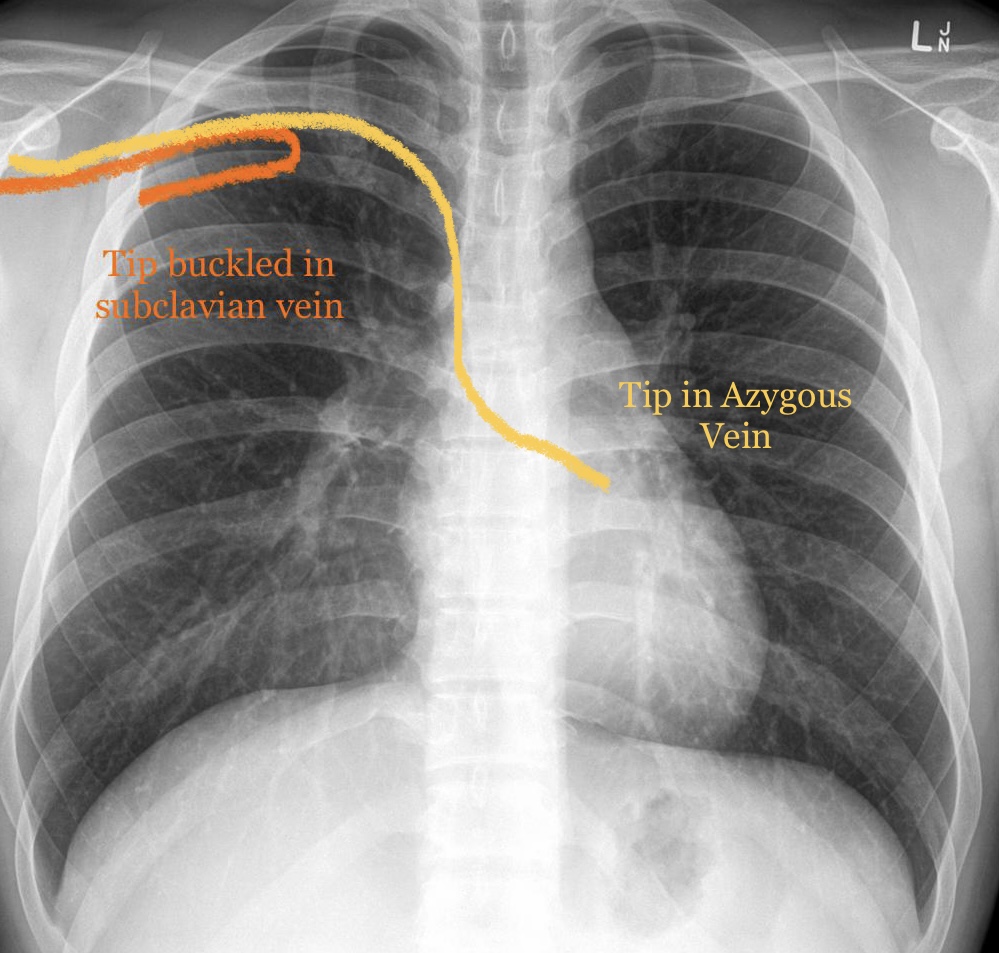
20/
Incorrect Positions:
Too high
Too low
Buckled in subclavian vein
Tip in Azygous
Tip in IJV
Tip in brachiocephalic vein
Incorrect Positions:
Too high
Too low
Buckled in subclavian vein
Tip in Azygous
Tip in IJV
Tip in brachiocephalic vein


• • •
Missing some Tweet in this thread? You can try to
force a refresh



