
Dr. Bhupesh Prusty: Herpes virus reactivation as a trigger for #MECFS and #LongCovid
Presenting data on how looking at results can generate different ideas for moving research forward
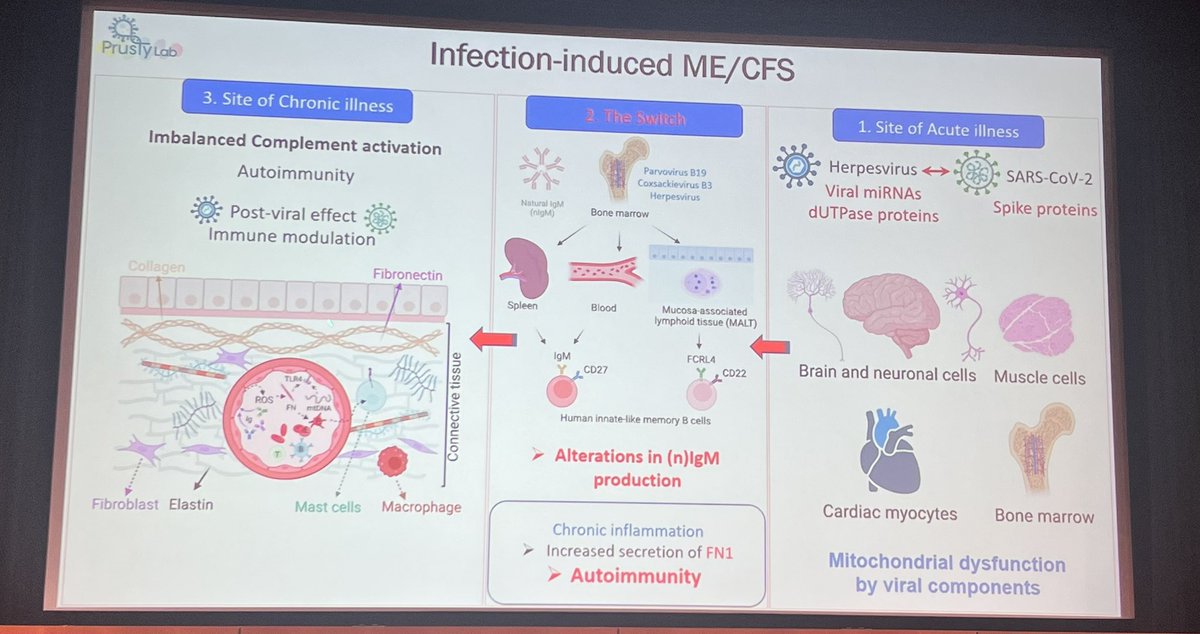
acute vs chronic contributors in mecfs: fibronectin, peripheral circulation, fibrobalst, mast cell. direct consequence of viral infection/reactivation in: brain and neuronal cells, muscle cells, cardiac myocites
brain muscles, cardia as site of acute disease, then indirect consequences as chronic illness manifested in symptoms such as pots, connective tissue disorder, etc based on the factors involved.
Study populations of #MECFS and No, mild, severe #LongCovid being studied vs healthy controls. #covidon, #napkon, #imme
herpesvirus signature in #mecfs and #longcovid immunoglobin detection in pt serum using proteins against herpesvirus dUTPase proteins HSV-1 dUTPase found in over 50% of long covid pts
Autophagy is inhibited under these conditions. Extensive mitochondrial effects are observed.
Autoimmunity is expected to play a role. Can we divide the pts into groups based on what antibodies they are expressing to find patterns? IgG pattern was not found. #mecfs pts have overlapping autoantibodies overlapping with SLE and MS.
IgM against autoantigens can differentiate mecfs patients from healthy controls
Most mecfs pts have increased IgM response against a lot of environmental and common pathogenic antigens
3 very important proteins are depleted in activated immune complex of mecfs patients
serum fibronectin and significantly increased in #MECFS and #LongCovid - it tells us that there is an alteration in the clotting process. The amount of fibronectin correlates with severity.
Both cellular and plasma fibronectin is increased in mecfs
Reaching pathological concentrations of serum fibronectin is easier in females than males.
In a 1995 study of mice, 3 weeks post infection, fibronectin levels went up and IgM-FN1 decreased, this was reversed 4 weeks post infection.
IgM fibronectin can be a natural IgM (doesn't require an antigen). Their job is to clean when cells die. autoimmunity is highly correlated with this type of IgM.
Looking at 2 of the most common natural IgMs (PC and MDA) and you see the same pattern in #LongCovid and #mecfs with these additional natural IgMs
biochemical overlapping of #MECFS and #LongCovid patients is high when comparing FN1
pts that most commonly develop long covid where not hospitalized. This is due to an inhibition of sars-covid-2 expression with the re-activation.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



