
Hey #medicine residents !!
Time to talk about EOSINOPHILS today. Not as common a consult as thrombocytopenia and anemia but important nonetheless.
A short 🧵 to touch upon all things eosinophilia 👇🏻
#MedTwitter
Time to talk about EOSINOPHILS today. Not as common a consult as thrombocytopenia and anemia but important nonetheless.
A short 🧵 to touch upon all things eosinophilia 👇🏻
#MedTwitter

Before we go any further, it's important to know this
🩸Eosinophil ≥ 500 is ABNORMAL
Eosinophil is a predominantly tissue dwelling cell so 🩸 eosinophil DON'T correlate with tissue damage 🤷♂️
We see a few patients with ⤴️⤴️Eos and no 🫀🫁 injury !!
🩸Eosinophil ≥ 500 is ABNORMAL
Eosinophil is a predominantly tissue dwelling cell so 🩸 eosinophil DON'T correlate with tissue damage 🤷♂️
We see a few patients with ⤴️⤴️Eos and no 🫀🫁 injury !!
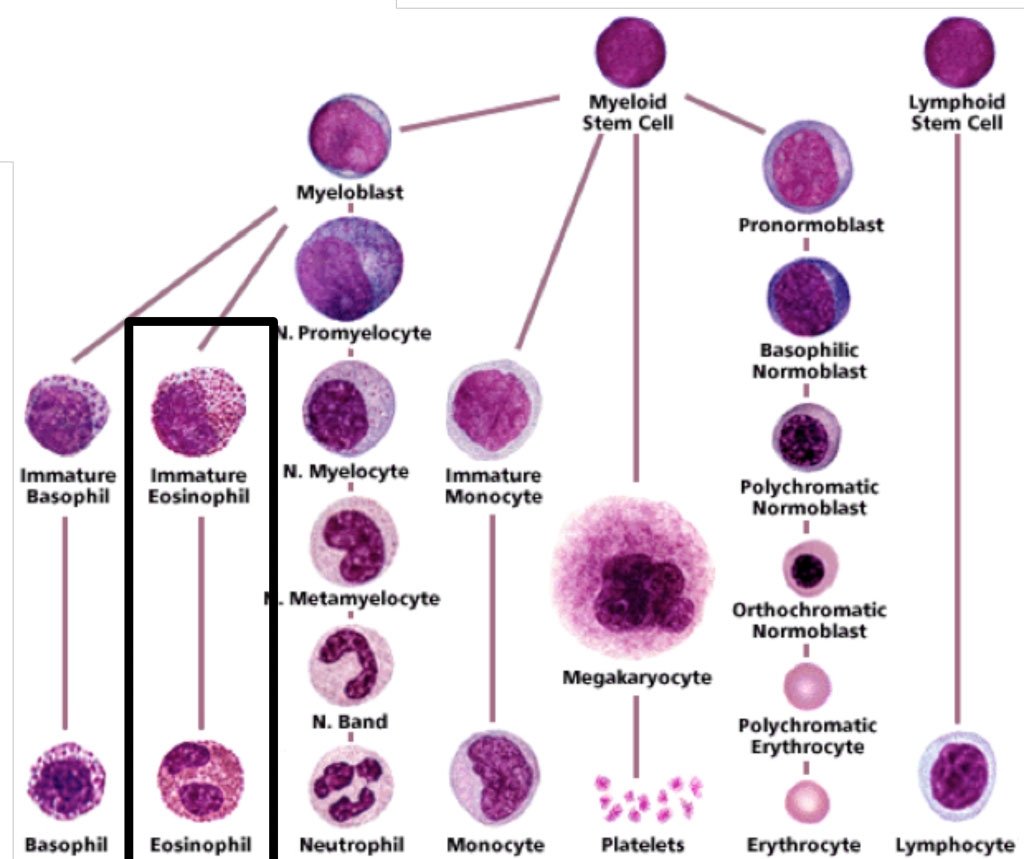
Where do eosinophils come from?
Short answer: Bone Marrow
They are cells of the granulocytic lineage, siblings of neutrophils and basophils, children of the myeloblast (image👇🏻)
IL5 is the cytokine responsible for it's production, important to know because we have anti IL5 mAb
Short answer: Bone Marrow
They are cells of the granulocytic lineage, siblings of neutrophils and basophils, children of the myeloblast (image👇🏻)
IL5 is the cytokine responsible for it's production, important to know because we have anti IL5 mAb
Why do we care about ⤴️⤴️ eosinophils?
Eos are GRANULAR cells and the granules contain toxic material.
⤴️Eos=⤴️ degranulation=⤴️toxic contents=🫁🫀🧠damage !!
Lots of reasons to bother 🙏🏻
Eos are GRANULAR cells and the granules contain toxic material.
⤴️Eos=⤴️ degranulation=⤴️toxic contents=🫁🫀🧠damage !!
Lots of reasons to bother 🙏🏻
Basics out of the way, let's start with the clinical bit.
What's your approach for ⤴️ eosinophils?
Start with a HISTORY 👇🏻
Drug history is very IMPORTANT. Always ask about complementary drug intake. This could be recent or remote.
Trust me, it's very important 🙏🏻
What's your approach for ⤴️ eosinophils?
Start with a HISTORY 👇🏻
Drug history is very IMPORTANT. Always ask about complementary drug intake. This could be recent or remote.
Trust me, it's very important 🙏🏻
So what are the other causes of ⤴️Eos?
•Allergies
•Parasitic infections
•Malignancies
•Immune disorders
The list is long and can be easily found over the internet !!
•Allergies
•Parasitic infections
•Malignancies
•Immune disorders
The list is long and can be easily found over the internet !!
What organs are most often affected??
•Skin
•🫁
•♥️
•🧠
•GI tract
Ask if the patient has a rash, cough, wheezing, palpitations, dyspnoea, diarrhoea etc.
On examination, look for enlarged nodes, liver and spleen !
•Skin
•🫁
•♥️
•🧠
•GI tract
Ask if the patient has a rash, cough, wheezing, palpitations, dyspnoea, diarrhoea etc.
On examination, look for enlarged nodes, liver and spleen !
These symptoms mean there's end organ damage and one needs to act quickly.
PERSISTENT ⤴️ eosinophils (≥1500/mcL) AND end organ damage = HES (Hypereosinophilic syndrome)
This could be d/t any cause and HES ≠ malignancy all the time.
i.e. the degree of ⤴️⤴️≠malignant cause.
PERSISTENT ⤴️ eosinophils (≥1500/mcL) AND end organ damage = HES (Hypereosinophilic syndrome)
This could be d/t any cause and HES ≠ malignancy all the time.
i.e. the degree of ⤴️⤴️≠malignant cause.
HES is a syndrome, one has to find the underlying cause.
HES could be d/t a myeloid neoplasm (M-HES), clonal lymphocytes (T-HES) or even be familial.
But most often our investigations don't reveal anything and we leave it at idiopathic HES 😭
#MedTwitter
HES could be d/t a myeloid neoplasm (M-HES), clonal lymphocytes (T-HES) or even be familial.
But most often our investigations don't reveal anything and we leave it at idiopathic HES 😭
#MedTwitter
Why is it important to recognise the underlying cause??
Well, to treat and prognosticate better.
M-HES for example is treated differently, it responds to imatinib and responds poorly to steroids 🤷♂️
#MedTwitter
Well, to treat and prognosticate better.
M-HES for example is treated differently, it responds to imatinib and responds poorly to steroids 🤷♂️
#MedTwitter
M-HES is due to a chromosomal rearrangement involving FIP1L1-PDGFRa, can be tested for by FISH.
Also a/w ⤴️ vitamin B12 and ⤴️tryptase, most often with splenomegaly.
If you suspect this, call your hematologist!!
Also a/w ⤴️ vitamin B12 and ⤴️tryptase, most often with splenomegaly.
If you suspect this, call your hematologist!!
More often than not, eosinophilia will be transient and secondary to drugs/infections. Will resolve with appropriate Rx and drug withdrawal 💪
What if it doesn't ??
Read along 👇🏻👇🏻
#MedTwitter
What if it doesn't ??
Read along 👇🏻👇🏻
#MedTwitter
Let's RECAPITULATE 👇🏻
•Hypereosinophila ≥ 1500/mcL
•HES is above + organ damage
•HES has many varieties, some are cancers
•MC organs involved 🫁♥️🧠, skin, GI tract
•Mostly transient, sec to infections/drugs
•If persistent, involve a hematologist
Moving on👇🏻
#MedTwitter
•Hypereosinophila ≥ 1500/mcL
•HES is above + organ damage
•HES has many varieties, some are cancers
•MC organs involved 🫁♥️🧠, skin, GI tract
•Mostly transient, sec to infections/drugs
•If persistent, involve a hematologist
Moving on👇🏻
#MedTwitter
Now let's talk LABS ✅
What do we order beyond the usual blood counts, metabolic panel, infection screen etc?
It depends on the symptoms and what the underlying suspected disease is !
Think of M-HES in a young male w/ ♥️ involvement, L-HES involves more of skin.
#MedTwitter
What do we order beyond the usual blood counts, metabolic panel, infection screen etc?
It depends on the symptoms and what the underlying suspected disease is !
Think of M-HES in a young male w/ ♥️ involvement, L-HES involves more of skin.
#MedTwitter
EGPA will present with 🫁 findings so tests depend upon clinical suspicious.
But we test with 2 things in mind, identifying the UNDERLYING CAUSE of HES and tests to IDENTIFY END ORGAN DAMAGE (eg Troponin)
#MedTwitter
But we test with 2 things in mind, identifying the UNDERLYING CAUSE of HES and tests to IDENTIFY END ORGAN DAMAGE (eg Troponin)
#MedTwitter
When do we treat URGENTLY ??
When there's severe organ damage like respiratory distress, other ♥️/🧠 symptoms !
That's just common sense🙏🏻
Admit and treat immediately.
Steroids are magical 🪄🪄🪄
#MedTwitter
When there's severe organ damage like respiratory distress, other ♥️/🧠 symptoms !
That's just common sense🙏🏻
Admit and treat immediately.
Steroids are magical 🪄🪄🪄
#MedTwitter
For most other situations, it's ok to initiate Rx on an outpatient basis.
Starting steroids before establishing a diagnosis is tricky business, must be avoided. It can change everything. Tread very carefully 🙏🏻
#MedTwitter
Starting steroids before establishing a diagnosis is tricky business, must be avoided. It can change everything. Tread very carefully 🙏🏻
#MedTwitter
If I urgently need to ⤵️ eosinophils, I use hydroxyurea while awaiting the test results.
Once the results are in, treat accordingly.
M-HES is treated with imatinib as imatinib 🚫PDGFR in addition to BCR-ABL1. The dose used here is <<CML (100mg OD)
#MedTwitter
Once the results are in, treat accordingly.
M-HES is treated with imatinib as imatinib 🚫PDGFR in addition to BCR-ABL1. The dose used here is <<CML (100mg OD)
#MedTwitter
If M-HES has ♥️ symptoms (usually does), start imatinib + steroids to avoid fatal myocardial necrosis 🙏🏻
For all other HES variants, the treatment is CORTICOSTEROID 🪄🪄🪄
#MedTwitter
For all other HES variants, the treatment is CORTICOSTEROID 🪄🪄🪄
#MedTwitter
The usual corticosteroid used is prednisolone at 1mg/kg.
Some use higher doses of methyl-pred like 1gm/d x 3 days. I use this dose only if severe symptoms or underlying autoimmune disease is the cause of HES.
#MedTwitter
Some use higher doses of methyl-pred like 1gm/d x 3 days. I use this dose only if severe symptoms or underlying autoimmune disease is the cause of HES.
#MedTwitter
How long to continue steroids??
Tricky question, continue till ANC ≤1500 & symptoms resolved and then taper.
If the patient needs >10mg steroids for the same, start a steroid sparing drug !!
What are those?
•Hydroxyurea
•Interferon a
•Mepolizumab
#MedTwitter
Tricky question, continue till ANC ≤1500 & symptoms resolved and then taper.
If the patient needs >10mg steroids for the same, start a steroid sparing drug !!
What are those?
•Hydroxyurea
•Interferon a
•Mepolizumab
#MedTwitter
Mepolizumab is an anti IL-5 monoclonal antibody
IL5 is required for eosinophil production so mepolizumab 🚫this.
Dosed at 300mg s/c once a month but it's not available in 🇮🇳 so our options are hydroxyurea > IFNa.
#MedTwitter
IL5 is required for eosinophil production so mepolizumab 🚫this.
Dosed at 300mg s/c once a month but it's not available in 🇮🇳 so our options are hydroxyurea > IFNa.
#MedTwitter
SUMMARY slide 💪💪
•Eos ≥1500/mcL w/ organ damage = HES
•HES has many variants
•M-HES treated differently from the rest (imatinib > steroids)
•All other HES variants are treated w/ corticosteroids initially f/b steroid sparing drugs if needed.
#MedTwitter
•Eos ≥1500/mcL w/ organ damage = HES
•HES has many variants
•M-HES treated differently from the rest (imatinib > steroids)
•All other HES variants are treated w/ corticosteroids initially f/b steroid sparing drugs if needed.
#MedTwitter
•Very often the underlying cause won't be identified = idiopathic HES.
If you read this far and learnt something, do share this thread 🧵
As always, thank you 🙏🏻🙏🏻
#MedTwitter
End.
If you read this far and learnt something, do share this thread 🧵
As always, thank you 🙏🏻🙏🏻
#MedTwitter
End.
• • •
Missing some Tweet in this thread? You can try to
force a refresh










